






Understanding the Essential Fatty Acids
George and Mildred Burr traversed the long roads leading from California to Minnesota in a Model T Ford Roadster in 1928, smuggling their two cages of Long-Evans rats into hotel rooms under overcoats to keep them safe from the fierce chill of the autumn nights. The recently married couple was about to revolutionize the world of nutrition by showing the essentiality of certain highly unsaturated dietary fats, and within two years would coin the term “essential fatty acids.”1
Over the ensuing decades, the consumption of vegetable oils rich in these fats more than doubled in the United States.2 The American Heart Association began recommending their use to lower cholesterol levels in 1961,3 and despite the Great Doubling that occurred during the Oiling of America, it recently recommended we nearly double our intakes yet again.4 Scientific research over the past several decades, however, has suggested that high intakes of these fats or imbalances between different classes of fatty acids may actually contribute to the risk of modern, degenerative disease. Just how essential, then, are the essential fatty acids? Are they double-edged swords? To begin putting the pieces of this puzzle together, let us return to the Burrs’ expedition to the cold, northern border where their rats would provide the first evidence of the essentiality of certain dietary fats.
The Discovery of the Essential Fatty Acids
George Burr had conducted his doctoral research in the deserts of Arizona and Utah, studying the effects of soil chemistry and climate on the distribution of plants and the quality of their sap. In September of 1924, having just finished this work, he left for the University of California, Berkeley, to study vitamin E with Herbert Evans, who had recently discovered the vitamin with Katherine Scott Bishop. The trip was serendipitous. Within a year, Burr married Mildred Lawson, the stock-keeper of Evans’ rats. Bishop and Evans were having trouble reproducing their vitamin E-deficient diet, and Burr helped them develop a highly purified diet using casein and sucrose. This diet, however, produced a deficiency that vitamin E could not cure. Evans thought they discovered a new vitamin, but Burr thought they discovered the essentiality of certain fats. In 1928, Burr left Berkeley for the University of Minnesota, where he was invited to continue his nutrition research as a professor of plant physiology. He left having discovered nothing of great importance about vitamin E, but having gained a life partner and having fortuitously stumbled upon a new deficiency disease to research.1
The possibility that certain dietary fats might be essential contradicted the conventional wisdom of the day. Since the discovery in 1845 that pigs are capable of synthesizing fat from carbohydrate, researchers believed that neither fats nor the fatty acids of which they are composed were essential nutrients.5 By the 1920s, most researchers believed that the only function of fats was to store excess energy and to carry fat-soluble vitamins. In 1920, Osborne and Mendel showed that rats consuming a diet containing only 0.3 percent fat consumed more food and grew more vigorously than rats on a standard diet and concluded that “if true fats are essential for nutrition during growth the minimum necessary must be exceedingly small.”6 The diets were made of meat residue and purified starch and contained brewer’s yeast and alfalfa as sources of vitamins. Now that we are in the midst of an obesity epidemic, we may look back on this paper and suggest that it showed an advantage of including some fat in the diet in order to properly regulate appetite. Its significance at the time, however, was to show that fat-soluble vitamins are required for growth but that fat itself is not.
The diet the Burrs used to produce essential fatty acid deficiency was very different from the diet Osborne and Mendel used. The Burrs purified casein through repeated rounds of precipitation and purified sugar through repeated rounds of crystallization. They used yeast to supply B vitamins, a fat-free extract of cod liver oil to supply vitamins A and D, and in some experiments they used a fat-free extract of wheat germ to supply vitamin E. When they fed this diet to young, growing rats, the rats developed irritated, sore and scaly skin, dandruff, and hair loss. Their tails were inflamed, swollen, scaled and rigid, and were hemorrhaging in certain spots (Figure 1). Their kidneys degenerated and blood appeared in their urine. The females stopped ovulating and became infertile. Rats of both sexes drank massive amounts of water, yet did not urinate any more than the control rats, suggesting the water simply evaporated right out of their skin. Despite eating much more food, they gained much less weight; after several months they began to lose weight and within six months to a year they all had died.7-8
Figure 1. Tails of Essential Fatty Acid Deficient and Normal Rats
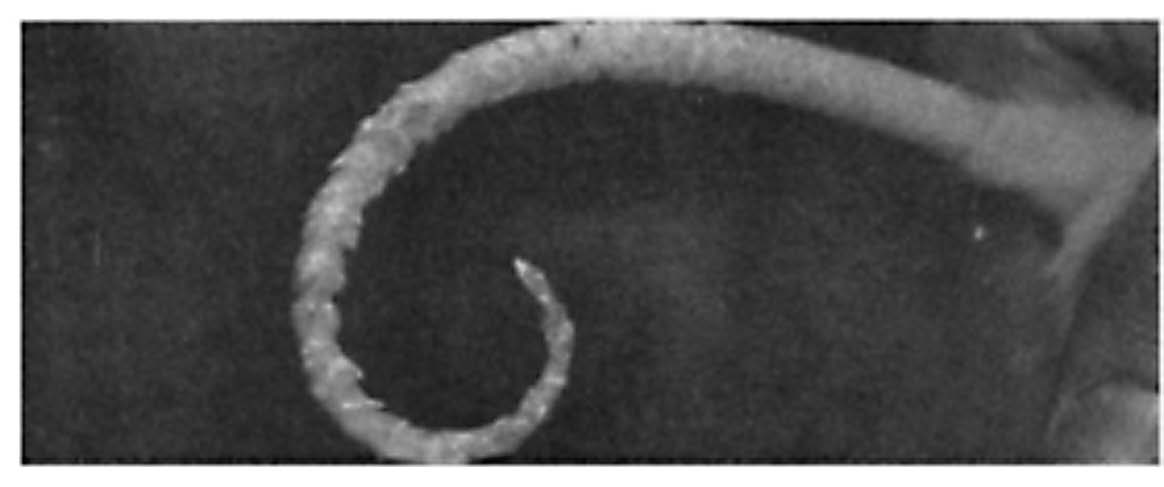 a. This rat was fed the essential fatty acid deficient diet without a curative oil. Its tail is plagued by dermatitis and scaly lesions.
a. This rat was fed the essential fatty acid deficient diet without a curative oil. Its tail is plagued by dermatitis and scaly lesions.
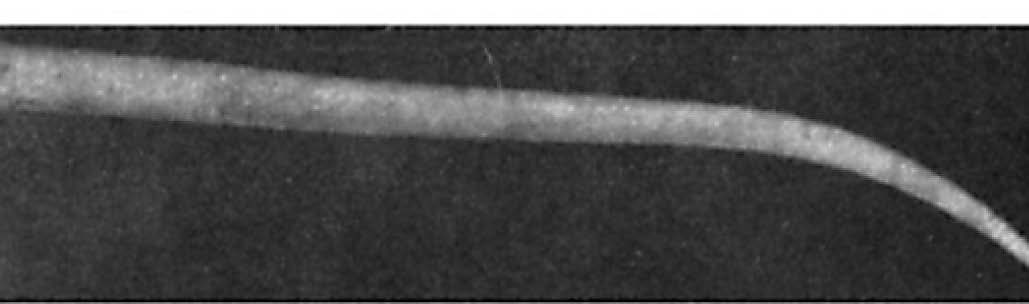 b. This rat was fed the essential fatty acid deficient diet supplemented with 0.4 percent of calories as PUFA provided by lard. Its tail is entirely normal in appearance.
b. This rat was fed the essential fatty acid deficient diet supplemented with 0.4 percent of calories as PUFA provided by lard. Its tail is entirely normal in appearance.
None of the vitamins cured the disease. Coconut oil, whether fully hydrogenated or not, could not cure the disease, and the curative effect of butter was very weak. The fatty acid fraction of cod liver oil helped lessen the symptoms and prevented the early death, while lard, liver, corn oil, flax oil and olive oil fully cured the disease. All of the effective oils had one thing in common: the presence of either linoleic acid or arachidonic acid, both of which are omega-6 polyunsaturated fatty acids (PUFAs).7-8 Later experiments showed that butter, which contains small amounts of both fatty acids, could fully cure the disease if provided in large enough amounts.9 Purified linoleic or arachidonic acids were each capable of fully curing the deficiency when provided alone.10 Arachidonic acid was at least three times more effective than linoleic acid, and probably would have proven to be even more effective had lower doses been used. Since our bodies use linoleic acid to synthesize arachidonic acid but do not use arachidonic acid to synthesize linoleic acid, this effectively demonstrated that only arachidonic acid is needed to cure the deficiency.
In the 1970s, researchers cured the dermatitis associated with essential fatty acid deficiency by topically applying prostaglandin E2 (PGE2) to the skin of deficient rats.11 PGE2 is a short-lived signaling compound that our bodies synthesize from arachidonic acid. It stimulates the formation of gap junctions12-13 and tight junctions,14 which are protein-based connections between cells whose vast array of functions includes regulating the permeability of the skin barrier.15-16 The skin of essential fatty acid-deficient rats not only evaporated copious amounts of water but also became permeable to lethal chemicals like barium sulfide, to which the skin is normally impermeable.17 Rats with genetic defects in gap junction formation develop scaly skin, increased permeability of the skin barrier, defective ovulation and infertility.15 Rats with genetic defects in tight junction formation exhibit excessive water loss through the skin.16 With either defect, most of the rats die soon after birth. Essential fatty acid deficiency therefore seems to be a result of our bodies having insufficient arachidonic acid available to synthesize the PGE2 needed to turn on the genes involved in forming critical junctions between cells.
How Essential Are the Essential Fatty Acids ?
The Burrs cured essential fatty acid deficiency in young, growing rats using 0.4 percent of calories as polyunsaturated fatty acids (PUFA) when provided by lard and 0.1 percent of calories when provided by liver.7 Evidence suggests the requirement is similar in human infants. This is discussed in more detail in the sidebar below. The essential fatty acid requirement, however, is influenced by other factors. The refined sugar used in these experiments increases the requirement.18 Vitamin B6 alone resolved the deficiency in later experiments by dramatically increasing the synthesis of arachidonic acid from linoleic acid stored in the tissues.19 Diets low in refined sugar and rancid vegetable oils, adequate in protein and total energy, and rich in vitamin B6, biotin, magnesium, and whole, fresh foods abundant in natural antioxidants are likely to reduce the essential fatty acid requirement to such a degree that it is impossible for a healthy, growing child under ordinary circumstances to develop a deficiency.
The requirement in adults is likely to be even lower. Researchers at the University of Wisconsin Madison first tried to produce essential fatty acid deficiency in adult rats in 1947.20 The only way they were able to induce a deficiency was to starve the rats until they lost half their bodyweight. As they gained back the weight they had lost over the subsequent two months, they developed typical symptoms of essential fatty acid deficiency such as scaly skin and hair loss. A small amount of corn oil proved curative, but even in the deficient rats the symptoms disappeared when they returned to their original weight. It thus appears that most of the arachidonic acid required during growth is used to supply dividing cells with enough to store in their membranes, and to form junctions between newly generated cells. Adult rats, by contrast, can probably meet their much smaller needs for arachidonic acid even when they go long periods without any essential fatty acids in the diet by synthesizing it from the linoleic acid they have stored in their tissues.
George Burr’s first human guinea pig was his good friend and distinguished colleague Jesse F. McClendon.1 McClendon is best remembered as the first researcher to directly measure the pH of the human stomach, but he made substantial contributions to a number of fields including nutrition, cell membrane biology and invertebrate zoology. At the urging of White Castle owner Billy Ingram, he once conducted an experiment on a medical student, allowing the student to eat nothing but White Castle hamburgers and their associated buns and pickles for thirteen weeks. The student appeared to fair well on the diet and the study became a prominent feature of White Castle’s advertising.21 If only McDonald’s had been so lucky when Morgan Spurlock performed a similar experiment for his 2003 film Super Size Me. McClendon himself, however, had suffered from scaly skin and eczema between his fingers even in the absence of any potent hamburg-emia. At Burr’s urging, he cured the problem with a daily dose of corn or flax oil.1
Inducing an essential fatty acid deficiency in an adult human proved much more difficult than curing one. In 1938, the biochemist William Brown volunteered to go six months eating an extremely low-fat diet in Burr’s laboratory. Each day, he consumed three quarts of defatted milk, a quart of cottage cheese made from it, sucrose, potato starch, orange juice and some vitamin and mineral supplements. His blood lipids became more saturated and their concentrations of linoleic and arachidonic acids were cut in half. He experienced a marked absence of fatigue, his high blood pressure returned to normal, and the migraines he had suffered from since childhood completely disappeared.22 Rather than inducing a deficiency, the diet seemed to correct a long-standing excess, perhaps fueled by a history of vegetable oil consumption.
Dermatitis seemingly associated with essential fatty acid deficiency has occurred in adult humans on total parenteral nutrition (TPN), which is an intravenous infusion of a liquid diet. These diets were also deficient in vitamin K, iron, zinc, and various other trace elements, and essential fatty acids alone were never shown to resolve the dermatitis.23-24 TPN also involves a continuous infusion of glucose, which prevents the breakdown of adipose tissue and release of stored linoleic acid that would ordinarily occur between meals.25 All of the subjects receiving TPN, moreover, had severe underlying health problems, were often undergoing major gastrointestinal surgery, and were sometimes at the brink of death.
These disparate experiences highlight the likely variation that exists in vulnerability to essential fatty acid deficiency among adult humans. Alcoholism, diabetes, insulin resistance and certain genetic variations decrease the activity of delta-6-desaturase, one of the enzymes involved in the conversion of linoleic acid to arachidonic acid.26 Experiments in rats, moreover, suggest that the requirement during pregnancy and lactation is double that needed during the growth of young animals.27 Under ordinary circumstances, the requirement during adulthood is probably well below the minimum one could obtain from a diet made of whole foods. During pregnancy, periods of growth such as bodybuilding or recovery from tissue injury, or in disease states where existing PUFAs undergo oxidative destruction, the requirement may increase. People with low rates of arachidonic acid synthesis or strict vegetarians whose diets are devoid of arachidonic acid may be more vulnerable to essential fatty acid deficiency and may need higher intakes of linoleic acid. In these cases, borage oil or evening primrose oil can supply dihomo-γ-linolenic acid (DGLA), which is more easily converted into arachidonic acid than is linoleic acid, and liver or eggs yolks can supply arachidonic acid itself. These foods are likely to be more effective—and safer—than high intakes of linoleic acid.
The Essentiality of Omega -3 Fatty Acids
George Burr’s former graduate student, Ralph Holman, demonstrated in 1950 with his own graduate student, C. Widmer, that PUFAs are comprised of two separate families of fatty acids: linoleic acid is the precursor within the omega-6 family and is primarily converted in rat tissue to arachidonic acid, while alpha-linolenic acid (ALA) is the precursor within the omega-3 family and is primarily converted in rat tissue to docosahexaenoic acid (DHA).32 Omega-3 fatty acids improved weight gain to some degree in essential fatty acid deficient rats, but had no power to cure dermatitis, 32 infertility, or many other symptoms.17 In fact, omega-3 ALA made the dermatitis worse.19 The research community therefore ignored omega-3 fatty acids for decades. Once Ralph Holman and his colleagues convinced the medical establishment to include linoleic acid in intravenous TPN infusions, however, suddenly a new deficiency was born.
In 1982, Holman reported the first case of apparent omega-3 deficiency in a six-year-old girl who underwent repeated rounds of surgery for an abdominal gunshot wound and was maintained for over five months on TPN. The FDA had recently approved the addition of vegetable oils to TPN to provide linoleic acid, and two formulas were available: one containing safflower oil and one containing soybean oil.33 The safflower oil formula contained an omega-6-to-omega-3 ratio of one hundred fifteen, while the soybean formula contained a ratio of six, almost twenty times lower.34 After five months of the safflower oil formula, the girl experienced episodes of numbness, tingling, weakness, inability to walk, leg pain, psychological disturbances and blurred vision—symptoms that researchers had never seen in essential fatty acid deficient animals or in humans receiving fatfree TPN. Her blood levels of omega-3 fatty acids were low. When her physicians switched her to the soybean oil formula, her omega-3 fatty acid levels returned to normal and her neurological symptoms disappeared.
Animal experiments suggest that great excesses of linoleic acid are required to cause deficiencies in omega-3 fatty acids. In every organ, the concentration of DHA vastly outweighs the concentration of any other omega-3 fatty acid, but levels of DHA are especially high in the brain and retina, where its concentration is tightly regulated.35 In the early development of these tissues, small amounts of omega-3 fatty acids are required to provide maximal DHA content; after this window is closed, however, the brain and retina are very resistant to the effects of deficiency, just as mature animals and adult humans are resistant to the effects of arachidonic acid deficiency under ordinary circumstances.
Even during early development, however, great excesses of omega-6 linoleic acid are required to cause substantial decreases in the omega-3 DHA content of the brain and retina. When fed to weanling rats, the classic sucrose-casein essential fatty acid-deficient diet only depletes retinal DHA content by 15 percent. The addition of ten percent of calories as safflower oil, however, causes a much more dramatic 50 percent depletion.36 Feeding rats two percent of their calories as purified linoleic acid depletes the DHA content of the retina by 62 percent in the first generation and 92 percent in the second generation.37 Similar effects occur in the brain.38-39 Depletion of retinal and brain DHA using linoleic acid-rich vegetable oils causes visual and possibly learning defects in rats and rhesus monkeys.40-42
Our bodies use the same enzymes to convert ALA to DHA as they use to convert linoleic acid to arachidonic acid. A great excess of one precursor can therefore outcompete the other for the enzymatic machinery. Large amounts of any PUFA, moreover, will cause the cell to make less of this enzymatic machinery by convincing the cell that it is no longer needed.26 This competition and cellular confusion can be avoided altogether by providing small amounts of preformed arachidonic acid and DHA in the diet. Even though the concentration of DHA in breast milk is very small, the brains of breast-fed infants accumulate fifty percent more DHA than those of infants fed formulas devoid of the fatty acid.43 When a mother improves her DHA status by supplementing with cod liver oil during pregnancy and the first three months of lactation,44 it improves her child’s IQ at four years of age, although the effect is drowned out by other factors as the child grows older.45
The requirement for DHA is likely to be most critical during pregnancy, lactation, early development, and other periods of growth, tissue repair, or diseases involving the oxidative destruction of lipids.46 People who consume linoleic acid-rich vegetable oils are likely to have greatly decreased conversion of ALA to DHA. Since this is the norm on the standard American diet, most Americans eating a standard diet may be vulnerable to DHA deficiency. People who convert ALA to DHA poorly or strict vegetarians whose diets are completely devoid of DHA may benefit from consuming sources of preformed DHA such as cod liver oil or egg yolks from pastured chickens. Small amounts of cod liver oil are also useful in a broader range of circumstances to provide vitamins A and D.
The Omega -6-to -Omega -3 Ratio
An often-cited animal experiment suggested that the ideal ratio of omega-6 linoleic acid to omega-3 ALA is four-to-one, but this experiment injected rats with free fatty acids rather than feeding them dietary oils.47 A more realistic experiment that fed rats a mix of various vegetable oils in a broad range of different proportions showed that a ratio of nine-to-one maximized tissue DHA content just as well as lower ratios.48 The precise ratio is likely to be of much less importance, however, when there is preformed arachidonic acid and DHA in the diet. Nevertheless, people who consume the standard American diet rich in vegetable oils may face adverse consequences from consuming excess linoleic acid and people who consume large amounts of fatty fish, fish oil or cod liver oil may face adverse consequences from consuming an excess of the omega-3 fatty acid eicosapentaenoic acid (EPA).
Among ten populations studied from five different continents, American adults have the highest blood levels of omega-6 fatty acids and American infants have the lowest blood levels of omega-3 fatty acids.33 Up until the 1930s, Americans consumed on average about 15 grams (one tablespoon) of PUFA per day. Since the 1930s, this value has more than doubled to over 35 grams per day as Americans have increased their intake of vegetable oils rich in the omega-6 linoleic acid (see Figure 2).2 Most of this increase occurred after 1961 when the American Heart Association began recommending that people replace saturated fats with vegetable oils in order to lower cholesterol levels.3
Similar increases in linoleic acid have been shown to decrease the conversion of ALA to longer-chain omega-3 fatty acids such as DHA in humans.49 Human studies tend to look at the fatty acids incorporated into red blood cells, but animal experiments provide much more detailed information about the concentrations of fatty acids in the organs and glands where they are most needed. These experiments show that excesses of linoleic acid do not increase tissue concentrations of arachidonic acid; instead, they replace the true omega-3 DHA with a “fake” omega-6 version of DHA that ordinarily is not found in substantial amounts within the body.50 The main effect of the excess linoleic acid in the standard American diet is thus most likely to be a mild form of DHA deficiency.
The effect of excess linoleic acid is probably most detrimental to infants and young children whose brains are still developing. DHA deficiency during early development may have lasting effects on cognitive and visual function during adulthood. Animal experiments even suggest that these effects are multi-generational, with the DHA concentration of nervous tissue declining with each successive generation.
Even in adulthood, however, dietary fats influence the DHA concentrations of most other tissues. Recent research has shown that our tissues use DHA to synthesize compounds called “resolvins,” which are involved in bringing inflammatory responses to an end when they are no longer needed.51 Sufficient DHA thus allows the immune system to mount a robust inflammatory response against invading pathogens or damaged tissues and to bring the response quickly to an end once the task has been accomplished. Researchers are increasingly discovering that most degenerative diseases involve an element of chronic, low-level inflammation, and the inability to “turn off” important inflammatory processes once they are no longer needed could be part of the problem. DHA deficiency may therefore be at the root of widespread declines in cognitive function, increases in mental disorders and epidemic levels of degenerative disease.
EPA, a precursor to DHA, is an omega-3 fatty acid that accumulates in fish but generally exists in only infinitesimal quantities in mammals and other land animals. Many authors consider EPA an “anti-inflammatory” essential fatty acid, but its “anti-inflammatory” activity is a result of its ability to interfere with arachidonic acid metabolism. The conversion of arachidonic acid to PGE2 in immune cells is an important initiator of inflammation, but it also turns on the genes necessary for the synthesis of compounds that resolve inflammation, some of which are derived from arachidonic acid and others of which are derived from DHA.52 Providing sufficient DHA to allow the synthesis of the full spectrum of inflammation-resolving compounds is a nutritional approach to inflammation. Providing high doses of EPA that interfere with arachidonic acid metabolism, however, is a pharmacological approach, and it is likely to have many adverse consequences.
When Holman and Widmer first discovered the dichotomy between omega-3 and omega-6 fatty acids, they examined nine different tissues in rats on normal lab diets and could not find even a trace of EPA unless they had first induced essential fatty acid deficiency and all its related tissue damage.32 Several years later Holman conducted a study with another colleague showing that ALA aggravated essential fatty acid deficiency; if they gave the animals vitamin B6, however, the rats converted ALA to DHA rather than to EPA and the aggravating effect disappeared.19 More recent studies in humans have provided preliminary evidence suggesting that EPA interferes with growth in infants and immune function in adults, while DHA improves both growth and immune function.53-54
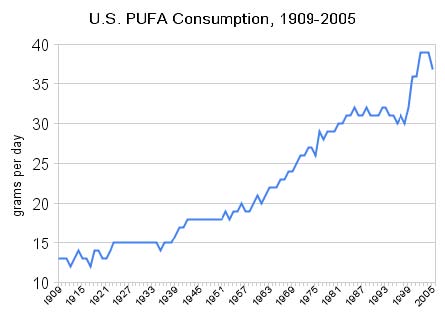 Figure 2. Increase in American PUFA Consumption
Figure 2. Increase in American PUFA Consumption
Consumption of polyunsaturated fat in the United States between 1909 and 2005 based on USDA food disappearance data. From reference 2, courtesy of Stephan Guyenet’s Whole Health Source blog (used with permission).
John Hughes Bennett, a nineteenth century Scottish physician who traveled the world studying the use of cod liver oil in medicine, wrote in his Treatise on Cod Liver Oil that excessive doses over extended periods of time could cause gastrointestinal problems, excessive menstrual bleeding, itchy skin eruptions and excessive evaporation of water through the skin.55 The last three symptoms seem very much like the hormonal disruptions, hemorrhaging and skin problems known to occur during arachidonic acid deficiency. Had the Burrs looked for gastrointestinal disorders during essential fatty acid deficiency, they probably would have found them. Non-steroidal anti-inflammatory drugs (NSAIDs) work their magic by interfering with the production of PGE2 from arachidonic acid, a characteristic they share with EPA. One of the most common set of side effects associated with these drugs is gastrointestinal disturbances. Four out of ten users of NSAIDs experience symptoms such as heartburn, acid reflux, stomach burning, nausea, or bloating.56 Researchers have used NSAIDs to produce food intolerances in mice that result in a form of severe intestinal damage called villous atrophy that is usually associated with celiac disease,57 suggesting that a deficiency of arachidonic acid or the PGE2 made from it may underlie celiac disease and other food intolerances, perhaps by preventing the gut from forming cellular junctions and thus impairing its integrity. Excessive doses of EPA from fatty fish, fish oil and cod liver oil may contribute to all of these symptoms in susceptible individuals.
Our bodies use the same enzymes to convert EPA to DHA as they use to convert ALA to DHA or linoleic acid to arachidonic acid. The same conditions that reduce the requirement for arachidonic acid and DHA are likely to increase a person’s tolerance for EPA. A diet that excludes refined sugar and rancid vegetable oil, is low in total PUFA content, is adequate in protein and total energy, and is rich in vitamin B6, biotin, calcium, magnesium, and fresh, whole foods abundant in natural antioxidants should not carry any risk of arachidonic acid deficiency when moderate amounts of EPA are consumed. Liberal amounts of egg yolks and liver providing preformed arachidonic acid would provide extra insurance against damage by EPA. Under these conditions, it would be safe to consume cod liver oil—valuable for its abundant provision of DHA, vitamin A and vitamin D—in spite of its EPA content.
The Perils of PUFA: Oxidative Stress
In 1985, the lipid researcher Hugh Sinclair gave a pre-banquet speech on his seventy-fifth birthday before the Second International Congress on Essential Fatty Acids, Prostaglandins and Leukotrienes in London, in which he described the deleterious effects of one hundred days on an “Eskimo diet” of seal blubber and undeodorized mackerel oil. He went on the diet to measure his bleeding time because the weather during a recent trip with several colleagues to northwestern Greenland had curtailed him from measuring the bleeding times of real Eskimos. Despite a daily supplement of vitamin E, his blood and urine levels of malondialdehyde (MDA)—a product of the oxidative destruction of PUFA (see Figure 3d)—rose to fifty times the normal level. Although MDA causes birth defects, Sinclair was not worried about having “misshapen offspring” because his sperm had disappeared.31
Sinclair’s experience illustrates one of the unique dangers of all essential fatty acids, regardless of their class—their vulnerability to oxidative stress.
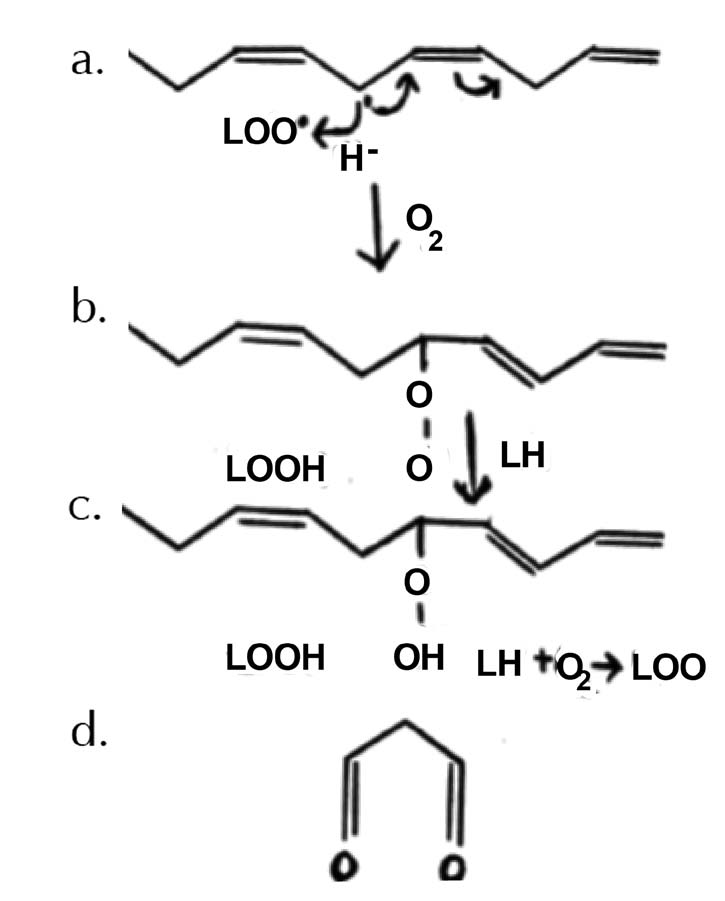 Figure 3. Oxidative Stress and the Shattering of Delicate PUFAs
Figure 3. Oxidative Stress and the Shattering of Delicate PUFAs
a. Compounds with unpaired electrons, called free radicals, are capable of stealing electrons from, or “oxidizing,” PUFAs. PUFAs are uniquely vulnerable to oxidation because they are the only fatty acids with two or more double bonds, and it is the carbon that lies directly between two double bonds that is vulnerable to oxidation at physiological temperatures. In the figure, a lipid peroxyl radical (LOO) steals an electron and a hydrogen atom from a PUFA.
b. Having stolen the electron and hydrogen atom, the lipid peroxyl radical becomes a lipid peroxide (LOOH). The addition of oxygen to the oxidized fatty acid forms a new lipid peroxyl radical that can oxidize another PUFA (LH).
c. There are now two lipid peroxides, one shown in its chemical structure and one abbreviated as LOOH. The newly oxidized fatty acid (L•) can now continue the chain reaction.
d. Many of these oxidized fatty acids will continue to degenerate into smaller compounds, like a glass that shatters into many pieces. One such compound, malondialdehyde (MDA), is shown in the figure. MDA is particularly dangerous because it can leave the membrane and damage proteins, DNA, and other important cellular structures. This process can be likened to the shattering of delicate glass, which results in a mess of dangerous shards that must be properly cleaned up.
Oxidative stress, or lipid peroxidation, shown in Figure 3, can be thought of as the destruction of structurally and functionally important molecules within the body, beginning with the shattering of PUFAs. PUFAs, in this sense, are like delicate glass. Glass performs many useful functions: we use it to protect ourselves and our property from the assaults of raging storms, for the utensils from which we eat and drink, to see when our vision fails, to examine complex specimens whose details we cannot otherwise distinguish with the naked eye, and in many other more sophisticated examples of modern technology. At the same time, glass is delicate and can shatter. When glass shatters, it invariably leaves behind a mess of dangerous shards. Anyone who breaks a glass on their kitchen floor knows to clean up the shards immediately, lest they or their family cut their feet by walking on them. Likewise, when PUFAs shatter they leave behind shards such as MDA, which are capable of damaging proteins, DNA and other structurally and functionally important components of our cells.
The best way to avoid shattering glass is to be careful with how one uses, cleans and stores it. Nevertheless, the danger of breaking glass will increase simply by having too much of it around. Likewise, the consumption of excess PUFAs increases oxidative stress even when the oils are fresh and properly cared for. Consumption of fresh, non-oxidized DHA, EPA or omega-3-rich perilla oil increases markers of oxidative stress in rats.58 Rats fed 30 percent of their diet as corn oil have double the rate of lipid peroxidation, half the aerobic capacity, and 42 percent lower glycogen stores in their heart tissue compared to rats fed an equal amount of coconut oil.59 A randomized, double-blind, placebo-controlled trial likewise showed that six grams per day of fish oil increased lipid peroxides and MDA in healthy men, regardless of whether they were supplemented with 900 IU of vitamin E (see Figure 4).60
Sinclair might have better replicated the “Eskimo diet” had he sought the guidance of an Eskimo. Arachidonic acid is necessary for sperm production, and the liberal consumption of glands and other organs rich in arachidonic acid may protect the Inuit and Aleut peoples from the high levels of EPA they obtain from fatty fish and marine oils.31 There may be other components of their traditional diets that limit the vulnerability of PUFAs to oxidative stress, such as antioxidants like coenzyme Q10, lipoic acid, and preformed vitamin A found abundantly in organ meats, or other unknown factors. Human studies have generally used alpha-tocopherol, a form of vitamin E, to protect against the oxidation of fish oils within the body, but supplements of pure alpha-tocopherol suppress levels of gamma-tocopherol, a different form of vitamin E with a unique spectrum of antioxidant protection. Some of the main oxidants in human blood, moreover, are water-soluble so PUFAs require water-soluble antioxidants such as vitamin C for protection. Exactly which components of the traditional Inuit diet best protected them from their high intake of fish oils is unclear, but Sinclair’s experience demonstrates the danger of attempting to replicate a particular peculiarity of one group’s traditional diet without replicating the diet as a whole.
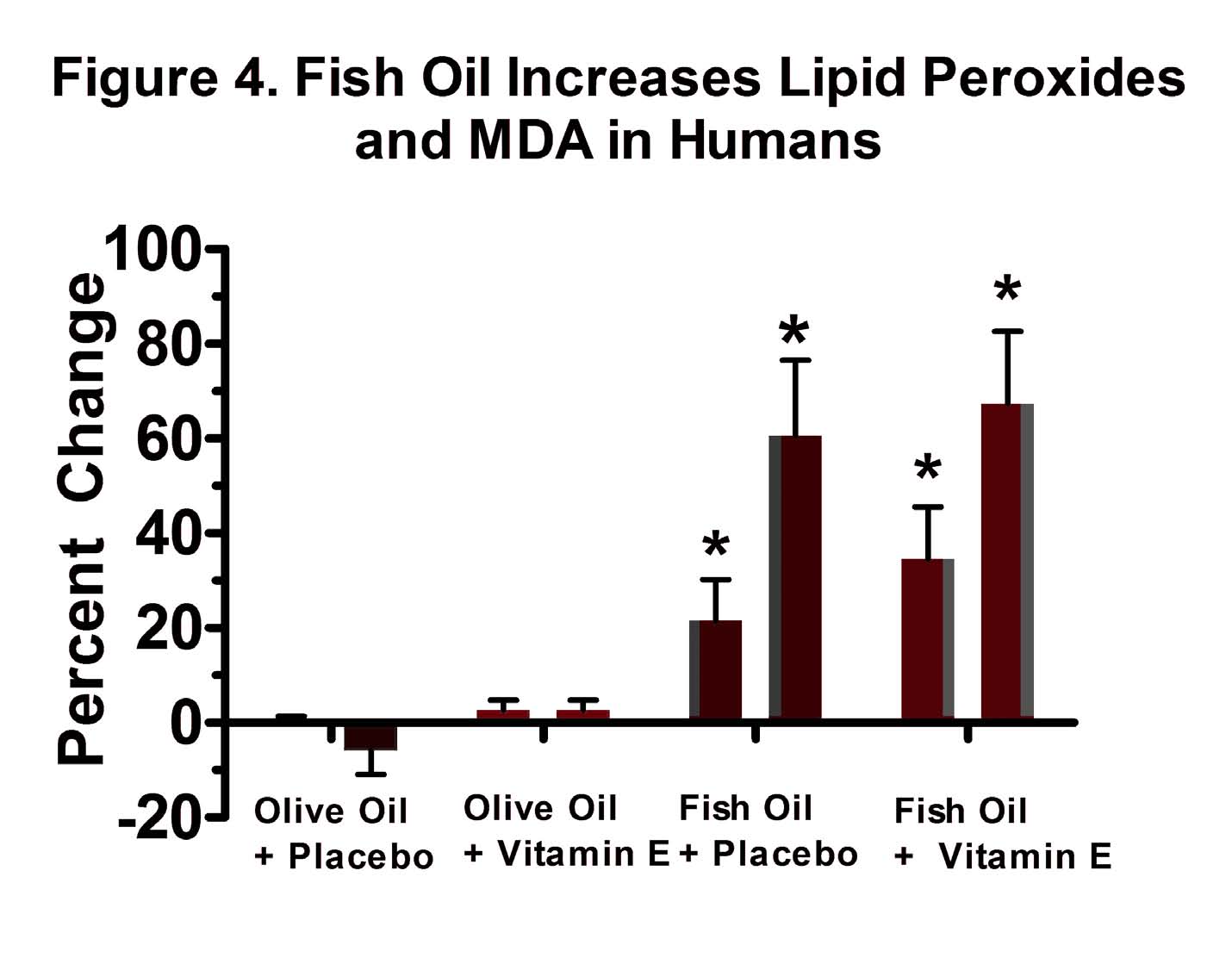 Figure 4. Fish Oil Increased in Lipid Peroxides and MDA in Humans While Vitamin E Had No Effect
Figure 4. Fish Oil Increased in Lipid Peroxides and MDA in Humans While Vitamin E Had No Effect
A double-blind, randomized, placebo-controlled trial compared six weeks of supplementation with six grams per day of omega-3 fatty acids from menhaden fish oil to supplementation with six grams per day of olive oil, with or without 900 IU per day of vitamin E as synthetic alpha-tocopherol, in healthy men. For each group, the bar on the left represents the change in lipid peroxides, and the bar on the right represents the change in MDA. Asterisks indicate a statistically significant increase over the course of the six weeks. Fish oil supplementation caused a significant increase in lipid peroxides while MDA and vitamin E had no effect. Adapted from the data in reference 60.
Do Vegetable Oils Prevent Heart Disease ?
While the amount of essential fatty acids required to prevent deficiency diseases may be nearly infinitesimal under most conditions, it may be possible that the optimal amounts are much higher. Research, however, suggests quite the opposite: even though the medical establishment has recommended the consumption of vegetable oils to prevent heart disease for decades, randomized, controlled trials conducted in humans demonstrated conclusively that vegetable oils cannot decrease atherosclerosis and suggested that they probably cause cancer.
Experiments in the 1950s showed that “milk shakes” with their natural fats removed and replaced with vegetable oils could lower cholesterol levels in humans when compared to “milk shakes” filled with saturated fats.61-62 A number of researchers suggested that replacement of traditional saturated fats with the newfangled vegetable oils would decrease the risk of heart disease by decreasing cholesterol levels and thereby decreasing the accumulation of atherosclerotic plaque.
The American Heart Association criticized this hypothesis in 1957 because no research had yet shown that making such a substitution could actually prevent the occurrence of a heart attack. A five-member ad hoc committee chaired by Irvine Page authored the report, concluding that it would be “premature” to act on the hypothesis that heart disease results from insufficient polyunsaturated oils and that research should focus on the actual diseases of atherosclerosis, heart attacks, and strokes rather than presumed surrogate markers like serum cholesterol.63 Four years later, the state of the evidence remained the same but three members of the committee were dropped and replaced by four new members, including Ancel Keys, a leading proponent of the theory that dietary animal fat causes heart disease. The updated report recommended that men who are overweight, have high blood pressure or high cholesterol, lead “sedentary lives of relentless frustration,” or have a strong family history of heart disease should replace part of the saturated fat in their diets with polyunsaturated fat.3
In the ensuing years, many researchers published trials of dietary fat substitution, but most of them were poorly designed and poorly controlled. Only six randomized, controlled trials specifically testing the substitution of polyunsaturated vegetable oils for animal fats have been published.64-69 These trials are discussed in more detail in the sidebar below. None of the trials showed that replacing traditional animal fats with polyunsaturated vegetable oils could lower mortality. Instead, the studies suggested that such a substitution increases the risk of cancer after a period of about five years and may increase the risk of heart disease as well.
 Figure 5. The Oxidation of LDL, Not Its Concentration, Determines Atherosclerosis
Figure 5. The Oxidation of LDL, Not Its Concentration, Determines Atherosclerosis
The open circles represent non-oxidized LDL and the filled circles represent LDL in which the PUFAs of the outer membrane have been oxidized. The vertical axis shows the absolute amount of LDL taken up by immune cells called macrophages. The horizontal axis shows the concentration of LDL with which the macrophages were incubated. The concentrations used are below what is found in human blood. The uptake of non-oxidized LDL reaches an early plateau, and a five-fold increase in concentration has virtually no effect on the amount of LDL taken up by the macrophages. The oxidation of LDL, by contrast, increases the uptake five-fold, and the uptake continues to increase as the concentration of oxidized LDL in the medium increases. This suggests that the concentration of non-oxidized LDL in the blood has no effect on the formation of atherosclerotic plaque, while the oxidation of PUFAs in the LDL membrane likely promotes atherosclerosis. Figure from reference 72.
In March of 1984, Time Magazine released a cover story entitled “Hold the Eggs and Butter,” announcing that “cholesterol is proved deadly” and lauding the American Heart Association for having been right all along in suggesting that we should banish fatty animal foods from our diet in favor of polyunsaturated oils.70 The AHA had recommended this for 23 years and finally, the authors proclaimed, there was scientific evidence to prove the case. This scientific evidence, however, had nothing to do with eggs and butter. The National Institutes of Health had hoped to create a massive, double-blind study replacing animal fats with polyunsaturated oils, but abandoned the project after two years, claiming that the diets did not lower cholesterol levels as much as they expected. They then conducted what went down in history as the Coronary Primary Prevention Trial, successfully lowering the risk of heart disease using cholestyramine, a drug that increases the conversion of cholesterol to bile acids. However, the reduction in heart disease mortality was offset by an increase in deaths from cancer, accidents and other causes, so that total mortality remained unchanged. The study was nevertheless widely hailed as having finally proved that cholesterol causes heart disease.
Three months later, the Proceedings of the National Academy of the Sciences published a critical paper that the media completely ignored.71 One of the authors was Daniel Steinberg, who chaired the NIH Consensus Conference later that December. The Consensus Conference provided official government sanction to the proclamation that cholesterol had been proven deadly. Steinberg’s paper showed that the critical change in the LDL particle that renders it toxic to the cells lining the blood vessel walls is the oxidation of the PUFAs in its outer membrane. The same authors showed that cells of the immune system called macrophages would take up oxidized LDL, but not non-oxidized LDL, in a concentration-dependent manner (see Figure 5).72 Later experiments showed that the components of the oxidized LDL particle that turn on specific genes causing macrophages to turn themselves into the fatty “foam cells” that populate atherosclerotic plaques, are oxidized derivatives of linoleic acid.73
The obvious implication of these studies is that the oxidative destruction of PUFAs in the LDL membrane, but not the concentration of cholesterol carried in the blood by these LDL particles, determines the development of atherosclerosis. It is no wonder, then, that trials attempting to prevent heart disease with diets rich in polyunsaturated vegetable oils failed so miserably.
Do Fish Oils Prevent Heart Disease?
Researchers in the 1970s suggested that the high content of omega-3 fatty acids in the diet of the Greenland Inuit may have protected them from heart disease by lowering their cholesterol and triglyceride levels.75 Since then, dozens of randomized, controlled trials have tested the effect of fish oil supplementation on total and cardiovascular mortality, discussed in more detail in the sidebar below. These studies suggested that about one gram of long-chain omega-3 fatty acids per day may prevent arrhythmia in patients prone to chronic heart failure or in patients recovering from a recent heart attack. They also suggested that long-term use of fish oils for more than four years may actually increase mortality from heart disease and all causes.
Many other groups eating traditional diets appear to be free or nearly free of heart disease, and a high intake of marine oils is not a universal trait of these diets. The main source of fat for the Masai, for example, is highly saturated butterfat. The inhabitants of Tokelau consume a diet based mostly on coconut and to a lesser extent on seafood, and even the seafood they prepare contains only two percent of its calories as long-chain omega-3 fatty acids.76 The inhabitants of Kitava consume about two percent of their total calories as omega-3 fatty acids,77 which is greater than the amount that Tokelauans consume but much lower than the amount that the Inuit consume. The traditional diet of Crete provides most of its fat as saturated butterfat from cheese and as monounsaturated olive oil, and contains very little fish.78 If we are to offer a hypothesis about what protects all these groups from heart disease, we must first identify what their traditional diets share in common. The most obvious place to start is the complete absence of refined foods. A very high intake of marine oils, by contrast, is a specific peculiarity of the Inuit diet.
Back to Traditional Diets
Experimental evidence shows clearly that the requirement for essential fatty acids is infinitesimal under most conditions and can be easily met by eating a diet that includes traditional whole animal foods without necessarily adding any specific fats or oils. There is very little evidence to suggest that consuming higher amounts of these fatty acids under ordinary conditions is health-promoting.
At the same time, many foods containing PUFAs provide other important nutrients. The Inuit, for example, obtained vitamin D from fatty fish and marine oils. Inland-dwelling Inuit who did not have access to these foods were vulnerable to disorders of calcium deficiency.82 These included fits of involuntary muscle contractions called tetany, and a type of hysteria called pibloktoq in the native language. Pibloktoq involves several days of irritability or withdrawal, a sudden excitation wherein the victim flees the camp and engages in irrational and dangerous behavior, convulsive seizures, a twelve-hour period of coma or stuporous sleep, and a final return to normal. It would be absurd to argue that the Inuit should have avoided the fatty fish and marine oils that helped prevent these conditions simply because they provided omega-3 fatty acids in great excess of the amount needed to promote health.
The most common plant foods Weston Price mentions in Nutrition and Physical Degeneration are the banana and sweet potato, but he also reported the use of cereal grains and legumes among many groups, and other authors have reported the use of substantial amounts of nuts and seeds among the Australian Aborigines. These foods would provide an excess of linoleic acid, but would also provide a broad spectrum of other useful nutrients. All of the groups Price studied consumed organ meats, which reduces the risk of an imbalance between omega-3 and omega-6 fatty acids by providing preformed arachidonic acid and DHA, and may supply critical antioxidants necessary to protect excess PUFAs from oxidizing within the body. The use of a single component of these diets such as nuts and seeds or high-dose fish oil without the use of other components such as organ meats, however, may provoke the ravages of imbalanced PUFA intake and oxidative stress.
The need for essential fatty acids increases during childhood, bodybuilding, recovery from injury, chronic disease states, pregnancy and lactation. During these times, the use of foods such as liver and egg yolks from pasture-raised animals and small amounts of cod liver oil is especially important. Some individuals may, for unknown reasons, require higher intakes of essential fatty acids. Symptoms of deficiency are shown in Figure 6 and can be used to determine whether someone might benefit from increasing their intakes of these foods. Rather than denouncing the essential fatty acids as “toxic” because they can promote inflammation or oxidative stress, they should be seen as delicate and precious nutrients that must be handled properly, taken in appropriate amounts, and taken within the context of a traditional diet rich in a broad spectrum of nutrient-dense foods. Within this context, the essential fatty acids will promote robust, radiant and vibrant health.
SIDEBARS
SUMMARY: UNDERSTANDING THE ESSENTIAL FATTY ACIDS
• The primary essential fatty acids are the omega-6 arachidonic acid and the omega-3 DHA.
• Arachidonic acid is found in liver, egg yolks, and other fats from land animals, and in small amounts in seafood. DHA is found in cod liver oil, fatty fish, and in smaller amounts in the organs and fats of land animals.
• Symptoms of arachidonic acid deficiency include dry, scaly and itchy skin, hair loss, dandruff, reproductive difficulties, gastrointestinal disturbances, and food intolerances. Symptoms of DHA deficiency include numbness, tingling, weakness, pain, psychological disturbances, poor cognitive function, difficulty learning, and poor visual acuity. Deficiencies of both fatty acids contribute to poor growth, poor immunity, and inflammation.
• The requirement for essential fatty acids is likely to be well below 0.1 percent of calories on a diet that is devoid of refined sugar and rancid vegetable oils, low in polyunsaturated vegetable oils, adequate in protein and total energy, and rich in vitamin B6, biotin, calcium, magnesium, and fresh, whole foods abundant in natural antioxidants.
• The requirement for essential fatty acids is lowest in healthy adults and highest in infants and growing children, pregnant and lactating women, bodybuilders, people recovering from injury, and people with chronic disease. Alcoholism, diabetes, insulin resistance, certain genetic variations, and strict vegetarianism may make someone more likely to become deficient. Additional liver, egg yolks, and cod liver oil can be used to correct deficiencies.
• Excess linoleic acid from vegetable oils can cause a deficiency in DHA. An excess of the omega-3 fatty acid EPA from fish and cod liver oil can cause a deficiency in arachidonic acid. For this reason, cod liver oil should be used in moderation and in combination with a diet rich in egg yolks and organ meats.
• Essential fatty acids are vulnerable to a process called oxidation, which can cause cellular damage.
• Replacing traditional animal fats with polyunsaturated vegetable oils may increase the risk of heart disease, cancer and total mortality.
• One gram per day of omega-3 fatty acids from fish oil reduces cardiovascular mortality in patients with chronic heart failure or who have recently had a heart attack. However, fish oil may increase cardiovascular and total mortality, especially when used for more than four years in combination with a standard modern diet.
• The liberal use of organ meats and egg yolks combined with small amounts of cod liver oil renders the essential fatty acids safe and health-promoting.
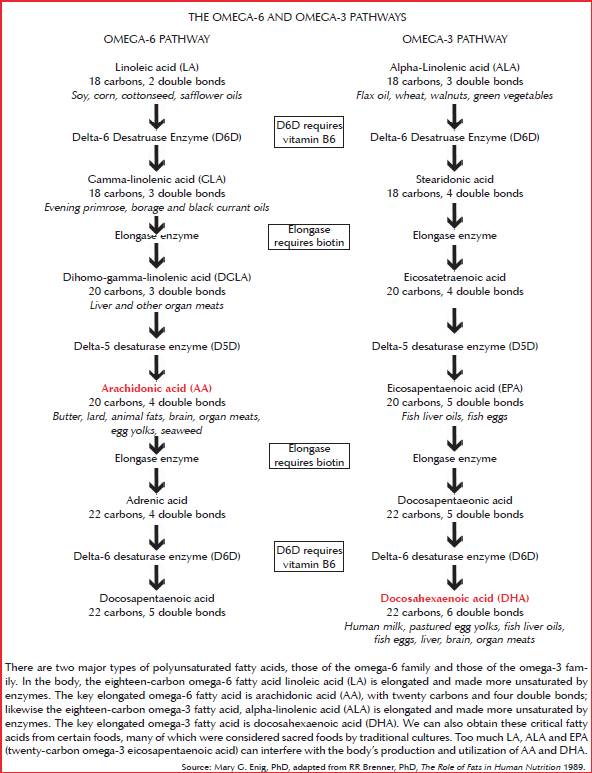
THE OMEGA-6 AND OMEGA-3 PATHWAYS
There are two major types of polyunsaturated fatty acids, those of the omega-6 family and those of the omega-3 family. In the body, the eighteen-carbon omega-6 fatty acid linoleic acid (LA) is elongated and made more unsaturated by enzymes. The key elongated omega-6 fatty acid is arachidonic acid (AA), with twenty carbons and four double bonds; likewise the eighteen-carbon omega-3 fatty acid, alpha-linolenic acid (ALA) is elongated and made more unsaturated by enzymes. The key elongated omega-3 fatty acid is docosahexaenoic acid (DHA). We can also obtain these critical fatty acids from certain foods, many of which were considered sacred foods by traditional cultures. Too much LA, ALA and EPA (twenty-carbon omega-3 eicosapentaenoic acid) can interfere with the body’s production and utilization of AA and DHA.
Source: Mary G. Enig, PhD, adapted from RR Brenner, PhD, The Role of Fats in Human Nutrition 1989.
How Essential Are the Essential Fatty Acids ? A More Detailed Look
The requirement for essential fatty acids is, under most conditions, exceedingly small. This should not be surprising; after all, if we require omega-6 fatty acids because we need enough arachidonic acid to allow our body to convert into signaling compounds as it needs them, then arachidonic acid fills a role similar to that of vitamins A and D. We require several hundred micrograms per day of vitamin D and several milligrams per day of vitamin A. To put this in perspective, we consume proteins, carbohydrates and fats in gram amounts. A microgram is one millionth of a gram and a milligram is one thousandth of a gram. We should therefore expect the requirement for essential fatty acids to constitute an extremely small percentage of our total energy intake.
Researchers who attempted to quantify the essential fatty acid requirement using purified fatty acids showed that just over two percent of calories as linoleic acid was needed to prevent deficiency in growing rats while less than 0.7 percent of calories as arachidonic acid was needed.10 Lower amounts of arachidonic acid may have proven effective had the researchers tested them. The Burrs did not use this approach. They used purified fatty acids to prove the point that the fatty acids themselves were curative, but used whole foods to quantify the requirement. “All workers,” they wrote, “recognize the fact that the acids isolated by the bromination method may not have exactly the same structure that they had in the natural oil.”8 The Burrs showed that the requirement was only 0.4 percent of calories when they used lard to cure the disease in growing rats and that the requirement was only 0.1 percent of calories when they used liver to cure it.7 Liver probably proved more effective than lard both because it is much richer in arachidonic acid and because it is rich in vitamin B6, which greatly enhances the conversion of linoleic acid to arachidonic acid.19
The essential fatty acid requirement seems to be similar in humans. Butter supplying 1.3 percent of calories as PUFA prevented poor growth, scaly skin and increased susceptibility to infections in human infants consuming a formula made partly from skim milk and mostly from corn syrup, but the investigators did not try using smaller amounts.28 The same authors reported that both 1.3 percent and 2.0 percent of calories as purified linoleic acid incorporated into a synthetic fat molecule cured eczema in infants fed the same type of formula.29 The requirement for purified linoleic acid in human infants fed a diet composed mostly of refined sugar is thus similar to the requirement in young, growing rats fed a similarly atrocious diet, which suggests that the essential fatty acid requirement in infants and growing children can be met by a diet providing less than 0.5 percent of calories as PUFA from animal fat, and much less than this if the fat is provided by liver.
One naturally wonders what the essential fatty acid requirement might be in people who are not consuming most of their calories as refined sucrose or corn syrup. In the 1960s, researchers compared the effect of starch-based and sucrose-based diets on PUFA metabolism. Both diets were deficient in essential fatty acids. The starch-based diet contained only 0.003 percent more calories as linoleic acid than the sucrose-based diet, but the rats fed starch had 50 percent more arachidonic acid and 80 percent more linoleic acid in their livers than the rats fed sucrose.18 Similarly, in essential fatty acid-deficient infants fed 80 percent corn oil, replacement of half the corn oil with hydrogenated coconut oil, which is completely devoid of PUFAs, substantially improved their eczema. High-sucrose diets increase lipid peroxidation in rats,30 a process that causes the destruction of essential fatty acids. Reducing refined sugar in the diet is therefore likely to sharply reduce the essential fatty acid requirement. A number of other factors may reduce this requirement as well, including biotin, vitamin B6, calcium, magnesium, avoidance of rancid vegetable oil, sufficient intake of protein and total energy, and a diet rich in fresh, whole foods abundant in natural antioxidants.31
Vegetable Oils and Heart Disease : A Closer Look
Six randomized, controlled trials specifically testing the effect of the substitution of polyunsaturated vegetable oils for animal fats on heart disease have been published.64-69
The first randomized, controlled trial of dietary fat substitution was published in 1965. Substitution of corn oil for animal fat and carbohydrate doubled the number of major cardiac events. The results were not quite statistically significant, meaning there was a slight possibility they were due to chance. The researchers concluded “that under the circumstances of this trial corn oil cannot be recommended as a treatment of ischaemic heart disease. It is most unlikely to be beneficial, and it is possibly harmful.”64
A second trial found that replacing animal fats with polyunsaturated vegetable oils increased mortality by 39 percent. Rather than considering the possibility that the lipid hypothesis might be false, the investigators concluded that “men who have had myocardial infarction are not a good choice for testing the lipid hypothesis.”66
Three other such trials found either no effect,65, 67 or a small increase in mortality in the group consuming vegetable oil, which was not statistically significant.68
The longest study on the effect of vegetable oil ever conducted was the Wadsworth Veterans Administration Hospital Study.69 The researchers randomized over four hundred men who were long-term inpatients to one of two dining halls. One hall used butter and the other used a mix of vegetable oils. The study was double-blinded and lasted over eight years. The researchers took care not to reuse the vegetable oil after cooking but took no such precautions with the butter, resulting in butter that was very deficient in vitamin E.74 There were also twice as many heavy smokers and 60 percent more moderate smokers in the butter group. The group consuming butter had 50 percent more cardiovascular deaths. The group consuming vegetable oil, however, had more atherosclerosis than the control group and in the last few years of the study began experiencing a marked increase in the risk of cancer. Total mortality was slightly higher among those consuming vegetable oil, but the difference was not statistically significant.
There are two remarkable findings about this study. Even though cardiovascular deaths were lower in the vegetable oil group, atherosclerosis slightly increased. This clearly disproves the hypothesis that vegetable oils decrease the accumulation of atherosclerotic plaque by decreasing cholesterol levels. It further suggests that had there been an equal distribution of smokers between groups and had the control group received adequate vitamin E, vegetable oil may have proven to markedly increase the accumulation of atherosclerotic plaque as well as the risk of cardiovascular mortality. The fact that cancer began rising in the vegetable oil group in the last few years of the study—again, despite the heavy rate of smoking and deficient intake of vitamin E in the control group—suggests that the full extent of the ravages of oxidative stress and inflammation caused by vegetable oils takes at least five years to develop. A longer study may have shown a much greater risk of mortality in the vegetable oil group. These six studies clearly show that vegetable oils are not capable of reducing total mortality and strongly suggest that they may raise the risk of heart disease and cancer.
Fish Oils and Heart Disease : A Closer Look
Dozens of randomized, controlled trials have tested the effect of fish oil supplementation and increases in the intake of fatty fish on total and cardiovascular mortality. Virtually all of them have been conducted in people with established heart disease taking drugs such as statins and aspirin, and most of them have lasted fewer than two years. In 2004, the Cochrane Collaboration published a massive review and meta-analysis of these trials.79 Meta-analyses pool the data of many studies together in an attempt to show the big picture and test whether methodological differences between trials or random chance are more likely to account for differences in results. When the authors pooled the data from forty-eight trials lasting longer than six months, the only effect that could be distinguished from chance was a reduced risk of heart failure. Fish oil provided no reduction in total or cardiovascular mortality.
Trials lasting less than one year were most likely to show positive results, while the only trial lasting more than four years—the Diet and Reinfarction 2 (DART 2) trial—showed a 15 percent increase in total mortality and a 30 percent increase in cardiovascular mortality. DART 2 used dietary advice to increase fatty fish intake in addition to fish oil supplementation, so could not be placebo-controlled or double-blind, and unfortunately funding problems led to interruptions of the recruitment process in the middle of the trial. Nevertheless, with over three thousand participants it was one of the largest fish oil trials ever conducted and, with over four years follow-up, it was the longest fish oil trial ever conducted. Thus, we should not casually dismiss the findings of this trial.
A recent meta-analysis brought to light eleven trials that were placebo-controlled and lasted more than one year.80 Pooling the data from these studies together showed that fish oil reduced the relative risk of cardiovascular death by 13 percent and reduced the relative risk of all-cause mortality by 8 percent.
The Italian GISSI-Prevenzione and GISSI-Heart Failure trials were the largest included in this meta-analysis and were responsible for most of the effect. These trials, together with the DART 1 trial, suggested that fish oil may prevent arrhythmia in patients with chronic heart failure and patients who have recently survived a heart attack.81 Researchers provided participants with roughly one gram of long-chain omega-3 fatty acids per day. The GISSI trials found a long-term benefit over the course of almost four years in heart failure patients but a much shorter-term benefit concentrated in the first year of the study in patients who had recently undergone a heart attack. The DART 1 trial similarly found an early benefit of fatty fish consumption and fish oil supplementation in patients who had recently suffered from a heart attack. Fish oil thus seems likely to prevent very specific types of heart failure rather than to prevent heart disease more generally.
None of these trials provided any evidence that healthy people benefit from taking fish oil or that doses higher than one gram of omega-3 fatty acids per day provide any benefit over smaller doses. The results of the DART 2 trial are particularly concerning because, like the results of the Wadsworth Veterans Administration Hospital Study (see sidebar on page 29), they suggest that high intakes of PUFAs may increase the risk of morbidity and mortality when consumed over the course of many years.
Figure 6. Symptoms of Essential Fatty Acid Deficiency
The following symptoms are based on a combination of animal and human evidence. Some of the symptoms are associated with severe deficiency and unlikely to be encountered under ordinary circumstances, and there are undoubtedly symptoms of each deficiency that are absent from the lists. These lists should help identify likely cases of essential fatty acid deficiency.
DHA Deficiency
• Numbness and tingling
• Weakness
• Pain
• Psychological disturbances
• Poor cognitive function and difficulty learning
• Poor visual acuity
• Blurred vision
• Poor immunity
• Poor growth
• Inflammation
Arachidonic Acid Deficiency
• Dry, scaly, and itching skin
• Hair loss
• Dandruff
• Reproductive difficulties in both males and females
• Gastrointestinal disturbances
• Food intolerances
• Kidney disease
• Inability to maintain weight
• Poor immunity
• Poor growth
• Inflammation
References
1. Holman RT. George O. Burr and the discovery of essential fatty acids. J Nutr. May 1988;118(5):535-540.
2. Guynet S. Have Seed Oils Caused a Multi-Generational Obesity Epidemic .Whole Health Source. http://wholehealthsource.blogspot.com/2010/04/do-seed-oils-cause-multi-generational.html. April 23, 2010. Accessed September 4, 2010.
3. Dietary fat and its relation to heart attacks and strokes. Report by the Central Committee for Medical and Community Program of the American Heart Association. JAMA. Feb 4 1961;175:389-391.
4. Harris WS, Mozaffarian D, Rimm E, et al. Omega-6 fatty acids and risk for cardiovascular disease: a science advisory from the American Heart Association Nutrition Subcommittee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Cardiovascular Nursing; and Council on Epidemiology and Prevention. Circulation. Feb 17 2009;119(6):902- 907.
5. Carpenter KJ HA. Evolution of Knowledge of Essential Nutrients. In: Shils ME ea, ed. Modern Nutrition in Health and Disease: Tenth Edition. Baltimore, MD; Philadelphia, PA: Lippincott Williams & Wilkins; 2006:3-9.
6. Osborne TB, Mendel LB. Growth on Diets Poor in True Fats. J Biol Chem. 1920;45(1):145-152.
7. Burr GO, Burr MM. A New Deficiency Disease Produced by the Rigid Exclusion of Fat from the Diet. J Biol Chem. 1929;82(2):345-367.
8. Burr GO, Burr MM. On the Nature and Role of the Fatty Acids Essential in Nutrition. J Biol Chem. 1930;86(2):587-621.
9. Holman RT. The ratio of trienoic: tetraenoic acids in tissue lipids as a measure of essential fatty acid requirement. J Nutr. Mar 1960;70:405-410.
10. Turpeinen O. Further Studies on the Unsaturated Fatty Acids Essential in Nutrition. J Nutr. 1938;15(4):351-365.
11. Ziboh VA, Hsia SL. Effects of prostaglandin E2 on rat skin: inhibition of sterol ester biosynthesis and clearing of scaly lesions in essential fatty acid deficiency. J Lipid Res. 1972;13:458-466.
12. Agrawal R, Daniel EE. Control of gap junction formation in canine trachea by arachidonic acid metabolites. Am J Physiol. Mar 1986;250(3 Pt 1):C495-505.
13. Civitelli R, Ziambaras K, Warlow PM, et al. Regulation of connexin43 expression and function by prostaglandin E2 (PGE2) and parathyroid hormone (PTH) in osteoblastic cells. J Cell Biochem. Jan 1 1998;68(1):8-21.
14. Blikslager AT, Roberts MC, Rhoads JM, Argenzio RA. Prostaglandins I2 and E2 have a synergistic role in rescuing epithelial barrier function in porcine ileum. J Clin Invest. Oct 15 1997;100(8):1928-1933.
15. Maass K, Ghanem A, Kim JS, et al. Defective epidermal barrier in neonatal mice lacking the C-terminal region of connexin43. Mol Biol Cell. Oct 2004;15(10):4597-4608.
16. Yuki T, Haratake A, Koishikawa H, Morita K, Miyachi Y, Inoue S. Tight junction proteins in keratinocytes: localization and contribution to barrier function. Exp Dermatol. Apr 2007;16(4):324-330.
17. Holman RT. Essential Fatty Acid Deficiency. A long scaly tale. Prog Lipid Res. 1968;9:275-348.
18. Casal JJ, Holman RT. The effect of kind of dietary carbohydrate upon the composition of liver fatty acids of the rat. J Am Oil Chem Soc. Dec 1965;42(12):1134-1137.
19. Witten PW, Holman RT. Polyethenoid fatty acid metabolism. VI. Effect of pyridoxine on essential fatty acid conversions. Arch Biochem Biophys. Dec 1952;41(2):266-273.
20. Barki VM, Nath H, et al. Production of essential fatty acid deficiency symptoms in the mature rat. Proc Soc Exp Biol Med. Nov 1947;66(2):474-478.
21. Minnesota Medical Foundation. A Look Back: Well Done. http://www.mmf.umn.edu/bulletin/2008/winter/lookback/index.cfm . Wineter, 2008. Accessed September 4, 2010.
22. Brown WR, Hansen AE, Burr GO, McQuarrie I. Effects of prolonged use of extremely low-fat diet on an adult human subject.1942; 16(6):511-523.
23. Holman RT. Omega-3 and Omega-6 Essential Fatty Acid Status in Human Health and Disease. In: Yehuda S, Mostofsky DI, eds. Handbook of Essential Fatty Acid Biology: Biochemistry, Physiology, and Behavioral Neurobiology. Totaway, NJ: Humana Press; 1997:139-182.
24. Fleming CR, Smith LM, Hodges MD. Essential fatty acid deficiency in adults receiving total parenteral nutrition. Am J Clin Nutr. 1976;29:976-983.
25. Wene JD, Connor WE, DenBesten L. The Development of Essential Fatty Acid Deficiency in Healthy Men Fed Fat-Free Diets Intravenously and Orally. J Clin Invest. 1975;1975(56):127-134.
26. Nakamura MT, Nara TY. Structure, function, and dietary regulation of delta6, delta5, and delta9 desaturases. Annu Rev Nutr. 2004;24:345-376.
27. Quackenbush FW, Kummerow FA, Steenbock H. The effectiveness of linoleic, arachidonic, and linolenic acids in reproduction and lactation. J Nutr. 1942;24(3):213-224.
28. Hansen AE, Wiese HF, Boelsche AN, Haggard ME, Adam DJD, Davis H. Role of linoleic acid in infant nutrition. Clinical and chemical study of 428 infants fed on milk mixtures varying in kind and amount of fat. Pediatrics. 1963;31(Suppl 1):171-192.
29. Hansen AE, Haggard ME, Boelsche AN, Adam DJ, Wiese HF. Essential fatty acids in infant nutrition. III. Clinical manifestations of linoleic acid deficiency. J Nutr. Dec 10 1958;66(4):565- 576.
30. Chaudhary DP, Boparai RK, Bansal DD. Implications of oxidative stress in high sucrose low magnesium diet fed rats. Eur J Nutr. Oct 2007;46(7):383-390.
31. Masterjohn C. How Essential Are the Essential Fatty Acids? The PUFA Report Part I: A Critical Review of the Requirement for Polyunsaturated Fatty Acids. Cholesterol-And-Health.Com Special Reports. 2008;1(2):1-25.
32. Widmer C, Holman RT. Polyethenoid Fatty Acid Metabolism. II. Deposition of Polyunsaturated Fatty Acids in Fat-Deficient Rats Upon Single Fatty Acid Supplementation. Arch Biochem. 1950;25(1):1-12.
33. Holman RT. The slow discovery of the importance of omega 3 essential fatty acids in human health. J Nutr. Feb 1998;128(2 Suppl):427S-433S.
34. Holman RT, Johnson SB, Hatch TF. A case of human linolenic acid deficiency involving neurological abnormalities. Am J Clin Nutr. Mar 1982;35(3):617-623.
35. Arterburn LM, Hall EB, Oken H. Distribution, interconversion, and dose response of n-3 fatty acids in humans. Am J Clin Nutr. Jun 2006;83(6 Suppl):1467S-1476S.
36. Forrest GL, Futterman S. Age-related changes in the retinal capillaries and the fatty acid composition of retinal tissue of normal and essential fatty acid-deficient rats. Invest Ophthalmol. Sep 1972;11(9):760-764.
37. Tinoco J, Miljanich P, Medwadowski B. Depletion of docosahexaenoic acid in retinal lipids of rats fed a linolenic acid-deficient, linoleic acid-containing diet. Biochim Biophys Acta. Mar 25 1977;486(3):575-578.
38. Mohrhauer H, Holman RT. ALTERATION OF THE FATTY ACID COMPOSITION OF BRAIN LIPIDS BY VARYING LEVELS OF DIETARY ESSENTIAL FATTY ACIDS. J Neurochem. Jul 1963;10:523-530.
39. Tinoco J, Babcock R, Hincenbergs I, Medwadowski B, Miljanich P. Linolenic acid deficiency: changes in fatty acid patterns in female and male rats raised on a linolenic acid-deficient diet for two generations. Lipids. Jan 1978;13(1):6-17.
40. Neuringer M, Anderson GJ, Connor WE. The essentiality of n-3 fatty acids for the development and function of the retina and brain. Annu Rev Nutr. 1988;8:517-541.
41. Neuringer M, Connor WE, Van Petten C, Barstad L. Dietary omega-3 fatty acid deficiency and visual loss in infant rhesus monkeys. J Clin Invest. Jan 1984;73(1):272-276.
42. Neuringer M, Connor WE, Lin DS, Barstad L, Luck S. Biochemical and functional effects of prenatal and postnatal omega 3 fatty acid deficiency on retina and brain in rhesus monkeys. Proc Natl Acad Sci U S A. Jun 1986;83(11):4021-4025.
43. Plourde M, Cunnane SC. Extremely limited synthesis of long chain polyunsaturates in adults: implications for their dietary essentiality and use as supplements. Appl Physiol Nutr Metab. Aug 2007;32(4):619-634.
44. Helland IB, Smith L, Saarem K, Saugstad OD, Drevon CA. Maternal supplementation with verylong- chain n-3 fatty acids during pregnancy and lactation augments children’s IQ at 4 years of age. Pediatrics. Jan 2003;111(1):e39-44.
45. Helland IB, Smith L, Blomen B, Saarem K, Saugstad OD, Drevon CA. Effect of supplementing pregnant and lactating mothers with n-3 very-long-chain fatty acids on children’s IQ and body mass index at 7 years of age. Pediatrics. Aug 2008;122(2):e472-479.
46. Calon F, Lim GP, Yang F, et al. Docosahexaenoic acid protects from dendritic pathology in an Alzheimer’s disease mouse model. Neuron. Sep 2 2004;43(5):633-645.
47. Yehuda S, Carasso RL. Modulation of learning, pain thresholds, and thermoregulation in the rat by preparations of free purified alpha-linolenic and linoleic acids: determination of the optimal omega 3-to-omega 6 ratio. Proc Natl Acad Sci U S A. Nov 1 1993;90(21):10345-10349.
48. Bourre JM, Dumont O, Pascal G, Durand G. Dietary alpha-linolenic acid at 1.3 g/kg maintains maximal docosahexaenoic acid concentration in brain, heart and liver of adult rats. J Nutr. Jul 1993;123(7):1313-1319.
49. Emken EA, Adlof RO, Gulley RM. Dietary linoleic acid influences desaturation and acylation of deuterium-labeled linoleic and linolenic acids in young adult males. Biochim Biophys Acta. Aug 4 1994;1213(3):277-288.
50. Bourre JM, Francois M, Youyou A, et al. The effects of dietary alpha-linolenic acid on the composition of nerve membranes, enzymatic activity, amplitude of electrophysiological parameters, resistance to poisons and performance of learning tasks in rats. J Nutr. Dec 1989;119(12):1880- 1892.
51. Serhan CN. Novel omega — 3-derived local mediators in anti-inflammation and resolution. Pharmacol Ther. Jan 2005;105(1):7-21.
52. Stables MJ, Gilroy DW. Old and new generation lipid mediators in acute inflammation and resolution. Prog Lipid Res. Jul 23 2010.
53. Carlson SE. Arachidonic acid status of human infants: influence of gestational age at birth and diets with very long chain n-3 and n-6 fatty acids. J Nutr. Apr 1996;126(4 Suppl):1092S-1098S.
54. Mebarek S, Ermak N, Benzaria A, et al. Effects of increasing docosahexaenoic acid intake in human healthy volunteers on lymphocyte activation and monocyte apoptosis. Br J Nutr. Mar 2009;101(6):852-858.
55. Bennett JH. Treatise on the Oleium Jecoris Aselli or Cod Liver Oil: BiblioBazaar; 1841. 56. Thiefin G, Rene-Marc F, Schaeverbecke T, Soufflet C, Barthelemy P. Characteristics and Impact of Upper GI Symptoms in Patients Treated with NSAIDs: Results of a Cross Sectional Epidemiological Study in Primary Care. Gastroenterology. 2008;134(4):A-734-A735.
57. Pecquet S, Prioult G, Campbell J, German B, Turini M. Commonly used drugs impair oral tolerance in mice. Ann N Y Acad Sci. Dec 2004;1029:374-378.
58. Saito M, Kubo K. Relationship between tissue lipid peroxidation and peroxidizability index after alpha-linolenic, eicosapentaenoic, or docosahexaenoic acid intake in rats. Br J Nutr. Jan 2003;89(1):19-28.
59. Diniz YS, Cicogna AC, Padovani CR, Santana LS, Faine LA, Novelli EL. Diets rich in saturated and polyunsaturated fatty acids: metabolic shifting and cardiac health. Nutrition. Feb 2004;20(2):230-234.
60. Allard JP, Kurian R, Aghdassi E, Muggli R, Royall D. Lipid peroxidation during n-3 fatty acid and vitamin E supplementation in humans. Lipids. May 1997;32(5):535-541.
61. Kinsell LW, Partridge J, Boling L, Margen S, Michaels G. Dietary modification of serum cholesterol and phospholipid levels. J Clin Endocrinol Metab. Jul 1952;12(7):909-913.
62. Ahrens EH, Jr., Blankenhorn DH, Tsaltas TT. Effect on human serum lipids of substituting plant for animal fat in diet. Proc Soc Exp Biol Med. Aug-Sep 1954;86(4):872-878.
63. Page IH, Stare FJ, Corcoran AC, Pollack H, Wilkinson CF, Jr. Atherosclerosis and the fat content of the diet. Circulation. Aug 1957;16(2):163-178.
64. Rose GA, Thomson WB, Williams RT. CORN OIL IN TREATMENT OF ISCHAEMIC HEART DISEASE. Br Med J. Jun 12 1965;1(5449):1531-1533.
65. Controlled trial of soya-bean oil in myocardial infarction. Lancet. Sep 28 1968;2(7570):693-699.
66. Woodhill JM, Palmer AJ, Leelarthaepin B, McGilchrist C, Blacket RB. Low fat, low cholesterol diet in secondary prevention of coronary heart disease. Adv Exp Med Biol. 1978;109:317-330.
67. Bierenbaum ML, Green DP, Florin A, Fleischman AI, Caldwell AB. Modified-fat dietary management of the young male with coronary disease. A five-year report. JAMA. Dec 25 1967;202(13):1119-1123.
68. Frantz ID, Jr., Dawson EA, Ashman PL, et al. Test of effect of lipid lowering by diet on cardiovascular risk. The Minnesota Coronary Survey. Arteriosclerosis. Jan-Feb 1989;9(1):129-135.
69. Dayton S, Pearce ML, Hashimoto S, Dixon WJ, Tomiyasu U. A Controlled Clinical Trial of a Diet High in Unsaturated Fat in Preventing Complications of Atherosclerosis. Circulation. 1969;150(1 Suppl 2):II-1-II-2.
70. Wallis C, Crooks C, Delayney P, Gribben S. Hold the Eggs and Butter. Time. 1984(March 26).
71. Steinbrecher UP, Parthasarathy S, Leake DS, Witztum JL, Steinberg D. Modification of low density lipoprotein by endothelial cells involves lipid peroxidation and degradation of low density lipoprotein phospholipids. Proc Natl Acad Sci U S A. Jun 1984;81(12):3883-3887.
72. Henriksen T, Mahoney EM, Steinberg D. Enhanced macrophage degradation of biologically modified low density lipoprotein. Arteriosclerosis. Mar-Apr 1983;3(2):149-159.
73. Nagy L, Tontonoz P, Alvarez JG, Chen H, Evans RM. Oxidized LDL regulates macrophage gene expression through ligand activation of PPARgamma. Cell. Apr 17 1998;93(2):229-240.
74. Dayton S, Hashimoto S, Rosenblum D, Pearce ML. VITAMIN E STATUS OF HUMANS DURING PROLONGED FEEDING OF UNSATURATED FATS. J Lab Clin Med. May 1965;65:739-747.
75. Bang HO, Dyerberg J, Hjoorne N. The composition of food consumed by Greenland Eskimos. Acta Med Scand. 1976;200(1-2):69-73.
76. Prior IA, Davidson F, Salmond CE, Czochanska Z. Cholesterol, coconuts, and diet on Polynesian atolls: a natural experiment: the Pukapuka and Tokelau island studies. Am J Clin Nutr. Aug 1981;34(8):1552-1561.
77. Lindeberg S, Berntorp E, Nilsson-Ehle P, Terent A, Vessby B. Age relations of cardiovascular risk factors in a traditional Melanesian society: the Kitava Study. Am J Clin Nutr. Oct 1997;66(4):845-852.
78. Christakis G, Severinghaus EL, Maldonado Z, Kafatos FC, Hashim SA. CRETE: A STUDY IN THE METABOLIC EPIDEMIOLOGY OF CORONARY HEART DISEASE. Am J Cardiol. Mar 1965;15:320-332.
79. Hooper L, Thompson RL, Harrison RA, et al. Omega 3 fatty acids for prevention and treatment of cardiovascular disease. Cochrane Database Syst Rev. 2004(4):CD003177.
80. Marik PE, Varon J. Omega-3 dietary supplements and the risk of cardiovascular events: a systematic review. Clin Cardiol. Jul 2009;32(7):365-372.
81. Burr ML, Dunstan FD, George CH. Is fish oil good or bad for heart disease? Two trials with apparently conflicting results. J Membr Biol. Jul 2005;206(2):155-163.
82. Wallace AFC. Mental Illness, Biology and Culture. In: Hsu FLK, ed. Pyschological Anthropology. Cambridge, MA: Schenkman Publishing; 1972:363-402.
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly magazine of the Weston A. Price Foundation, Fall 2010.
🖨️ Print post
I’ve just read about half of this article up to the paragraph about losing water through the skin. It occurs to me that this is why the USDA recommends drinking so much water. People are also willing to drink so much water without being instructed because they are so thirsty.
We are not told to ignore our sense of thirst, as we are to ignore hunger. In fact, we are told to go over the amount to satisfy thirst and force ourselves to drink too much.
I am completely lost on what course of action to take with fish oil supplementation. Please give me your advice on what you would do? I have used low doses for a few years now. Thank you for the great work you do.
Marc
I always knew fish oils (omega-3) where mostly anti-inflammation, and anti-free-radicals and that it competes for resources with the pro-inflammation omega-6s, but the point that fish oils cause Lipid Peroxides (free radicals) is a complete shocker!!!
Is the increase in Lipid Peroxides from fish oil due to the cooking of the fish? I.e. the pufa are being oxidized before consuming? Would sushi be the only way to avoid this?
Also since the average western diet is rich in pufas (omega-6), what should the corrective course of action be? Assuming a desired omega-6 to 3 ratio of 4:1 on a 2000 calorie diet?
Regarding the diets of (presumably healthy) groups around the world, wouldn’t another commonality be the higher consumption of saturated fats?
Great Work!
Wow, this has got to be one of the most detailed thorough works to date involving essential fatty acids. Thanks for all your hard work Chris.
Wow!
Just… wow, Chris! What a wonderfully thorough, detailed, and informative article. This is excellent work! Thank you for this.
“Supersize Me”
The White Castle study does not surprise me. I think Supersize Me greatly misrepresented what happened in the film. It was more a classist swipe at “the kind of people who eat at McDonald’s” (ie, lower-class Americans) than it was an attempt to be a real experiment of any sort.
The people he spoke to who ate all their meals at McDonalds were apparently slim and healthy, as was the White Castle study subject. What the filmmaker did was to stuff himself to the point of nausea three times a day, which is not what anyone does when they eat at McDonald’s.
But it was what people wanted to hear, that those people order too much food every time they go there, supersize their meal, and then force themselves to eat it all.
Besides the sheer calories he ate, he ended up consuming a huge amount of sugar and wheat. Who can say what was worse?
Brains?
Very nice article. I think instead of going off on my usual tirade about PUFAs I’ll just link to this article from now on.
One thing I have to wonder. The vast majority of a land-locked hunter-gatherer tribe’s omega 3 would be in the form of DHA from the brains of ruminants. Is it possible that all of the saturated fat and cholesterol in cow brains or WAP’s butter/cod liver oil is protective against lipid peroxidation?
Response to Lava, Tyler, Ben, Marc, Angela, Nathaniel, and Wyatt
Lava,
I do think that many people are not making enough PGE2 for maximal skin health, but another factor with the water is that the Institute of Medicine’s original proclamation meant this to include food water, and it has since been interpreted to refer only to added drinking water.
Tyler,
You’re welcome and thanks!
Ben,
Fish oils increase lipid peroxidation when they are fresh. The likely protective factors are the components of a healthy dietary context in which the fish oil is taken. The corrective course of action is to first and foremost roll back the linoleic acid intake by getting rid of modern vegetable oils. Saturated fat does seem to have some protective effect.
Marc,
I perosnally take small amounts of high-vitamin fermented cod liver oil. I think if your diet is good and you are taking one or fewer grams of omega-3 FAs from fish/cod liver oil per day you are probably fine.
Angela,
I mostly agree, and the experimental design makes both experiments intrinscially useless for drawing experimental conclusions, but I suspect that McDonald’s food is much worse today than White Castle’s food was then. That said, the experiment in SuperSize Me did use deliberate overconsumption of calories and also spread a lot of obvious misinformation from doctors, like the idea that blood triglycerides are mostly driven up by fat, when they are fairly well established to be mostly driven up by carbs, and plenty of other misinterpretation. Still, I thought it was an amusing historical anecdote.
Nathaniel,
You’re welcome and thanks!
Wyatt,
Thanks — yes, saturated fat probably has a protective effect, because it is fairly neurtral and it can displace excess carbohydrate. However, I doubt it is as important for protection as they classical essential antioxidants like vitamin C and E, glutathione-boosters, coenzyme Q10, and so on.
Chris
Corrections to my previous post!
(1) The USDA figures given for fat consumption from animal and vegetable sources were in pounds per YEAR not pounds per day!
(2) The Pubmed number for study regarding impairment of eNOS synthesis by LA (where the smiley face showed up) is 17696958.
(3) I failed to thank you, Chris,for providing such a great detailed explanation of PUFA requirements.
Jack C.
Chris,
Great article!
Under the topic of “Omega-6 to omega3 ratio” you said: “The main effect of excess linoleic acid is thus most likely to be a mild DHA deficiency”. This mild statement seems inconsistent with the your points regarding the correlation between LA intake and increased risk of cancer and CHD.
The data given in Figure 2 on the increase in PUFA consumption, in terms of grams per day per person is consistent with USDA data which shows that between 1960 and 2008, consumption of fats from vegetable sources increased from 41 to 77 pounds per person per day while during the same period, consumption of fats from animal sources decreased from 82 to 52 pounds per day. So the damaging effects of increased PUFA consumption was exacerbated by decreased consumption of healthy fats from animal sources.
A recent study (PMID 1769695smilies/cool.gif showed that linoleic acid impairs synthesis of endothelial nitric oxide synthase (eNOS) and thereby contributes reduces NO production which results in vascular constriction and reduced glucose metabolism. This contributes to obesity and endothelial dysfunction. Another study (PMID 15970594) found that myristic acid, a saturated fat, stimulates eNOS synthesis thereby enhances NO production and improves endothelial function. This is one of a number of mechanisms by which PUFA impairs and saturated fats improve endothelial function.
Regarding your point about PUFA and oxidative stress, the study “Linoleic acid increase lectin-like oxidized LDL receptor expression in human endothelial cells” (PMID 15855339) shows one mechanaim responsible for the increased oxidative stress caused by PUFA.
Two articles on the “Israeli Paradox”, PMID 8960090 and 17923822, offer a good overview of the increased CHD and cancer associated with high intake of n-6 fatty acids.
Jack Cameron
typo?
“Fish oil supplementation caused a significant increase in lipid peroxides while MDA and vitamin E had no effect.”
I think ‘MDA’ is a typo here. Perhaps ‘olive oil’ was meant?
Yes, there is a mistake, but that’s not what he meant. He wrote for Figure 4. “Fish Oil Increased in Lipid Peroxides and MDA in Humans While Vitamin E Had No Effect”. Therefore, at the end of the next paragraph he should have written the following. Fish oil supplementation caused a significant increase in lipid peroxides AND MDA WHILE vitamin E had no effect. The words AND and WHILE were transposed.
Thanks Chris!
Most exhaustive article on EFAs to date, at least that I know of. It was an enthralling reading, and a very welcome addition to my documentation on dietary fats and metabolism. Thanks a lot! Keep up the great work. Wizzu
Another magnum opus on EFAs
Chris,
Thanks for your continued excellent work on this subject. It’s such important information to get out there, as more and more people begin supplementing with (sometimes huge amounts of) fish oil.
Here’s another study that clearly shows that too much n-3 causes oxidative damage (more than any other fatty acid, including n-6): PMID: 8911273
“DHA deficiency during early development may have lasting effects on cognitive and visual function during adulthood.”
Do we know what types of defects in visual function? Are we talking myopia or some other defect? Thank you!
There’s not much left to eat
We can’t eat any simple carbs, we can’t eat fructose, we can’t eat grains or legumes, we can’t eat vegetable oils, we can’t eat many starchy tubers, we can’t eat many nuts and seeds, and we can’t eat many omega-6 rich animal fats.
And, oh yeah, now we can eat much omega-3 rich wild fish, wild game, and free-range beef or chicken.
I give up. 🙁
Paul, I can understand your food frustrations, but I’m curious why you are holding an opinion that “Fructose from ripe whole fruits, berries and melons are not acceptable for you…?
It’s my understanding and research that we are Cabin beings and the best choice and energetic food our 100 trillion cells require is the simplest carbon food from fruits as Frugivors, but I’m sure there are plenty who don’t subscribe to this science based type species…!
Last point about Fructose from nature is it’s the easiest to digest, assimilate, utilize and eliminate, as well does not involve the pancreas enzymatic process to be directly absorbed into the cells and produse ATP…!
RE: EFA’s, why was there a void of discussion regarding plant oils from; Flax, Chia, Hemp in this very special study report as factors of discovery…?
Not so obvious implication of the Steinberg, et. all study
Chris, after you explained the findings of the Steinberg study, you said:
“The obvious implication of these studies is that the oxidative destruction of PUFAs in the LDL membrane, but not the concentration of cholesterol carried in the blood by these LDL particles, determines the development of atherosclerosis.”
If you read Brian Peskin (yes, I know Mary says he’s a nut, but forget that for a moment and read him: ) His claim, and its totally logical, (and for all I know he has the studies that prove it), is that the PUFAs are not destroyed in the LDL, or anywhere in the body (gee, of course not, because that’s what Ray Peat claims and we KNOW THAT can’t be the case), but we are talking about mainly lenoleic acid that was oxidized WAY BEFORE it ever got into the plasma in the first place. Its just that the esters transporting the ruined PUFAs damage the arterial walls, whereas there would be no damage if the PUFA’s weren’t already adulterated before being picked up by the cholesterol.
So I’m just saying you’re right about everything (like that cholesterol is only the taxi-cab carrying the bad guys, but it doesn’t matter how many taxi’s are on the street), but double check on where you are claiming the damage takes place, ie where did the bad guys come from. Its very, very easy to see it taking place in the commercial handling of omega-6 oils. I still don’t see how someone can say it takes place in human physiology. Possibly it does in high concentrations, and you have the tests to prove that. But under normal intake, you’re not going to get oxidation of PUFA’s in the human body except in the specific processes they were designed to handle.
Regardless, the arterial damage has to be mostly caused by ingesting the adulterated PUFA’s, not by oxidation in vivo.
Thanks for considering this possibility.
Glenn A.
White Castle vs. Supersize Me
For starters, White Castle burgers are small. Intentionally small. Supersized meals at McDonalds are intentionally big. So comparing them is not apples to apples. And of course, we all know Michael Moore’s intent was not to present a factual, possible real life scenario, but to trash fast food.
I have always supplemented with Fish Oil, but not huge amounts, but I also have a diet which is rich in Fresh foods and Vegetables, Meat, and, in general, have a broad diet without a lot of repetition. Not too many carbs and flour products, either.
Thanks for the information. I finally understand why my fat phobe mom has such bad excema and bruising.
Chris,
Why does the WPA recommended doses of cod liver oil for pregnant women seem so high? Are they too high according to the info you provided? I am 2 weeks pregnant and about to start taking cod liver oil. I am going to buy Twin Labs until my Blue Ice fermented clo/butter oil comes in. I was taking it but it was Nordic Naturals Liquid which WPA says does not provide enough A & D and WORSE than that I just read the fine print: Vit E derived from REFINED Soybean oil which = GMO SOY. I am so mad at that company now, I have only been on that oil about a week. I hope my baby is okay.
I eat an excellent diet ( will be adding the liver and COl) but I eat butter, coconut oil, eggs ( pasture raised) , Grass Fed & Finished beef, pasture raised chicken, ALL organic veggies and fruits and all for years now and Absolutely NO GMO food of any sort.
Any info you can provide will greatly help, thank you!
@ Ivy Levinson
Pregnant women can generally take a higher dose of nutrients because a good portion of it goes to the developing child, rather than to the mother.
CLO also has a major benefit over fish oil: the vitamins, which also help protect the PUFAs from oxidizing. The vitamins are especially important for the child. Simply because of the vitamins, the recommended 2 teaspoons FCLO will cause you no problems given your current diet.
polyunsaturated/llard
Lard is 38-42 monounsaturated fat, under HOW ESSENTIAL ARE THE ESSENTIAL FATTY ACIDS: it states The Burrs cured essential fatty acid deficiency in young, growing rats using 0.4 percent of calories as polyunsaturated fatty acids (PUFA) when provided by lard and 0.1 percent of calories when provided by liver. Since only 6-10% is polyunsaturated fatty acids in lard, that means these rats were given enormous amounts of lard or the monounsaturated fatty acids were isolated? The article is 9,700 words long, the Declaration of Independence was 1337 words long and the Gettysburg address was 272 words long depending on which manuscript one had access to and after reading most of this article, I found myself saying like a mantra, “Be bold, Be brief, and Be gone.” Come on, Chris, surely brevity would be better than knee buckling, brain baking overkill! Essential fatty acids are not a deep subject, they’re simply fats we need, but not too much. Thomas Jefferson rewrote the Bible, and left out all the so called miracles, and what he ended up with was 28 pages. I think that was about 20 pages too long, but who’s to argue with TJ. Some of the information in this article is good, but much of it is confusing to many and far too long to hold one’s attention after five pages let alone 32 pages, not counting the references. I feel like I’m reading something out of congressional archives rather than what needs to be reader friendly relative facts. I give this article thumbs up for intent and thumbs down for not following what matters most when attempting to convey important data, “Keep it simple!” Essentially, you could have illustrated six or seven pictures with short references and everyone would have been informed, the point made, and much acheived. In other words, what I wanted was to know what works and what doesn’t, I don’t want to know how your thinking processes the science involved. If you go to NaturalNews, Mike Adams thing, and click Cartoons, you’ll understand one of the reasons NaturalNews is barely behind Mercola.com. With all your talent for research, the results put in clear and entertaining context would translate into a winning combination.
You’re not exactly brief yourself. Your reply is longer than the Gettysburg address as well. Though I admit it is entertaining I enjoy Cris’s prose as well.
Precious but Perilous
Chris Masterjohn’s article on fat in the new quarterly is terrific. Lay people have some trouble comprehending the syntax dynamic that is afoot in articles of this sort, the charts, the photos, etc., and sometimes one’s eyes, conscious mind and the arduous difficulty of connecting the dots get out of sync so one has to read carefully. Reading it twice or thrice helps, for instance, the arachidonic acid affect. First it causes inflammation and we get into microbial survival mode. Ultimately, it saves us when one goes traditional foods. At the end of the article, the lid is off absolutes and though we love our butter, lard, and tallow, sometimes animal fats are not the way to go. It’s much different for an Eskimo fighting the Arctic elements on 95% saturates and someone at a desk job in San Diego and shopping at a local market, health or mainstream. Our lifestyle ultimately determines our diet, which means fast food and the devastation thereof in many cases. That same San Diego resident, living in a city with weather to die for and not from, would certainly be better off, mentally and physically being a beachcomber, fishing in the Pacific, and growing a garden, but we’re slaves to an economy of lunacy, so, we must adhere to what pays the rent and not what makes sense, at least until we finally realize we’ve had enough. From Abraham Lincoln came two things:
“We may congratulate ourselves that this cruel war is nearing its end. It has cost a vast amount of treasure and blood. . . . It has indeed been a trying hour for the Republic; but I see in the near future a crisis approaching that unnerves me and causes me to tremble for the safety of my country. As a result of the war,
corporations have been enthroned and an era of corruption in high places will follow, and the money power of the country will endeavor to prolong its reign by working upon the prejudices of the people until all wealth is aggregated in a few hands and the Republic is destroyed. I feel at this moment more anxiety for the safety of my country than ever before, even in the midst of war. God grant that my suspicions may prove groundless.”
— U.S. President Abraham Lincoln, Nov. 21, 1864
(letter to Col. William F. Elkins)
The other of course came from the Gettysburg Address,
“Government by the people, of the people, and for the people shall not perish from the earth.”
But one other point we all need to remember is this:
“if all insects on Earth disappeared, within 50 years all life on Earth would end. If all human beings disappeared from the Earth, within 50 years all forms of life would flourish.”
― Biologist Jonas Salk
Thankfully, we have the Weston A. Price foundation, and Sally Fallon Morel and her great associates are making a difference. It’s alwaya a bottom up dynamic never from the top down and maybe someday we might remember what matters and ineffective the so called top actually is, they do more harm than good too often.
o3
hi, so i should be using fermented fish oils? what’s the best ratio of EPA to DHA in the capsule for? there are too many options and opinions out there. i dont know what to get. i just have one “molecularly distilled, ultra purified.” EPA-650mg and DHA 250mg. per serving.
i ran across this article while looking for a suggested dosage for the butter oil and fermented cod liver oil combination for my little 3-yr old granddaughter. it’s been suggested that it can help cure her cavity. i’m so overwhelmed with the info; but it makes me want to suggest not using it because now i am nervous….and not totally understanding what is being said. is the fermented with butter oil ok and the right ratio of omega 3’s and 6’s or would we be better off to not use it?
Hey Chris,
I know this article is quite old, but I was hoping you’re still checking in to respond to questions.
I am wondering what your take is on the essentiality of DGLA.
It seems you make a decent case among the articles you’ve written that DHA and Arachidonic are essential (whether from the diet or biosynthesized), LA and ALA are definitely not (that is, they are only insofar as they can produce DHA and arachidonic), and that EPA has questionable essentiality, but is likely not needed by terrestrial mammals (and likely only essential in marine life for structural purposes for cold adaptation). But I haven’t seen many comments from you on DGLA. Anecdotally many persons have seemed to respond nicely to GLA supplementation from EPO and/or Borage: things like hair growth, better skin, better mood, better digestion, and whatever else. Would you say that these benefits are mostly due to increasing biosynthesis of arachidonic acid? Or do you think DGLA has something unique and special to offer? Your one little comment in the article above makes it seem you definitely believe the former, that GLA and DGLA are just closer to arachidonic, hence why it is of benefit.
Article quote: [People with low rates of arachidonic acid synthesis or strict vegetarians whose diets are devoid of arachidonic acid may be more vulnerable to essential fatty acid deficiency and may need higher intakes of linoleic acid. In these cases, borage oil or evening primrose oil can supply dihomo-γ-linolenic acid (DGLA), which is more easily converted into arachidonic acid than is linoleic acid, and liver or eggs yolks can supply arachidonic acid itself. These foods are likely to be more effective—and safer—than high intakes of linoleic acid.]
I suppose people out there who feel they have benefited from GLA supplementation could switch to arachidonic acid and see what differences if any they experience. Of course, as of yet, arachidonic acid is not widely sold as a stand-alone supplement.
I’m a long-time reader of your material, but haven’t ever commented. But do know that many of us have really benefited from your work, which is in my estimate the most thorough and fair of any science writing I’ve come across.
I thank you for your thoughts.
-CP
Most interesting information here! In essence all the “star studies” that established food science (ILSI, Swedish SLV, EU,…) support its stance on 100% debunked!. I think you added the revisited Sydney heart study later.
Totally debunked is amazing! Only a month or so I read a serious article in a Swedish doctor magazine where the author listed both the Finnish and the Wadsworth veterans studies as two major well designed proofs that polyunsaturated fats promotes health while saturated fats promote disease!
I don’t recall if you or Stephan G. also debunked the “implicit proof” for that saturated fat creates Diabetes-2: “Saturated fat” Rat Chow. But one of you pulled out from the detailed ingredients list the 20% sugar mixed in, else the rats would not eat it. Like Ancel Keyes classified cakes as saturated fats for some of his less renowned betrayals.
But the reason I write this now is to hear what you regard as the best way to restore a healthy fat balance, starting of with a (presumed) excess pufas from years of following official advice.
I read about something called MDA -Malondialdehyde- which is formed as a break down product when pufas oxidize. In a study of prostate BPH and cancer, men were fed lycopene/tomatoes and at least in the first group MDA levels in plasma decreased. Still within 21 days study time only. The most interesting thing you pointed out about the Wadsworth study is that it can take some 5 years before cancer accelerates as a result of high pufa intake, depending of course at starting point. Snce MDA levels can be measured, high blood levels means high levels of PUFA oxidation while low that antioxidants are doing their job, or very low pufa levels in the body.
Could this be viable path to assess (cancer-) health in this respect ?
Regarding fatty acid turnover, how does it work ? In my case I eat a rather low carb diet and overcome effort angina shortly after I started it 3 years ago. There is still some visceral fat there and being only age 68 I want to “bullet proof” me for the next decade(s). What happens when I have exercised and just eat some coconut oil after? I saw drinking coffee + exercise would increase fatty acids dissolved in blood stream. Some would be consumed/burnt and some returned after.
I guess no partly rancid pufas would be taken up again by the tissues, at least if good fats were around in a normal body? Would pufas or satfats be taken up in preference? I guess any partly rancid fats would surely be left out of the tissues and be used for fuel in preference, but I don’t know. If you already have written about this, which would not surprise me at all, please point me in the right direction!
Keep up your really fantastic good work!
Are there any side effects of taking too much omega 3? According to http://www.ncbi.nlm.nih.gov/pubmed/11053532 there is. I have been taking cod liver oil for 2 years now and have been following the other dietary guidelines as well. Yet my bloodwork came back with a deficiency of AA and excess of omega 3 fats. The study really scares me. It suggests that too much omega 3 suppresses AA.
Any study’s results involving omega 6 oils such as safflower, sunflower, corn, etc. must be met with extreme skepticism due to the processing of those oils. Since it is not mentioned we must assume the researchers had no knowledge of the dangers of processed omega 6 oils. Peroxidation as mentioned in this report is much greater in open air than in the body. Furthermore, processing removes all benefits of the oils. Omega oils such as flax seed oil are never processed due to its high oxidation rate. This is from the findings of Brian Peskin a world class leader in PUFA’s. It would be interesting to find out the results if cold pressed unprocessed omega 6 oils were used instead. There is a study called the IOWA study where such oils were used. It compares the effects of fully functional PUFA’s vs that of fish oil.
About Peskin: https://www.westonaprice.org/health-topics/know-your-fats/brian-peskin-and-essential-fatty-acids/
Your chemical structures and arrow pushing in figure 3 are not correct. You should take the figure down or consider revising as it detracts from the quality of the article.