






 🖨️ Print post
🖨️ Print post
ARTICLE SUMMARY
- Stroke is the leading cause of disability and the third leading cause of death in the United States and most developed countries. There are two types of stroke: ischemic and hemorrhagic. The more common ischemic stroke results from blockage of a blood vessel supplying the brain, whereas the more damaging hemorrhagic stroke results from rupture of such a vessel.
- As cholesterol levels increase, the risk of hemorrhagic stroke decreases and the risk of ischemic stroke increases.
- Stroke mortality is lowest at cholesterol levels between 180 and 200. Mortality increases substantially below 180 and above 240. Mortality is highest below 160 and above 300.
- Although cholesterol itself does not cause stroke, a diet high in polyunsaturated fat and low in antioxidants can make LDL-cholesterol within the blood vulnerable to oxidation. Oxidized LDL can contribute to the development of stroke.
- High blood pressure is a far more important contributor to stroke than high or low cholesterol.
- Animal fat and fatty fish are associated with a lower risk of stroke. Polyunsaturated fat and carbohydrates are associated with a higher risk of stroke.
- Exercise, stress management, proper control of oral or systemic infections, and adequate nutrition can lower the risk of stroke. Important protective nutrients include magnesium, potassium, antioxidants and adequate protein.
Cholesterol is essential to human life. It is a primary constituent of cell membranes, essential to learning and memory, and the fundamental building block of bile acids, vitamin D, and the steroid hormones.1 Because in most cases the body synthesizes all the cholesterol it needs, however, scientists do not consider it an essential nutrient. Weston Price did not study the cholesterol content of primitive and modern diets, and he wrote his epic work, Nutrition and Physical Degeneration, decades before the medical establishment began measuring blood cholesterol levels and recommending cholesterol- lowering drugs and diets.2
Although Price’s work did not directly concern this vital molecule, the medical establishment’s campaign against it has nevertheless produced a nutritional paradigm that is antithetical to his findings: the American Heart Association, for example, recommends lowering cholesterol by limiting the consumption of butter, egg yolks, and organ meats – foods that formed the centerpiece of the primitive diets that Price’s work esteemed.3
Stroke Then and Now
Stroke is the third leading cause of death in the United States.4 Through the early 1990s, neither epidemiological studies5 nor controlled trials of cholesterol-lowering drugs6 were able to generate any evidence for an association between cholesterol levels and the risk of this disease. Today, however, the scene is very different. Recent news articles have reported that cholesterol-lowering drugs do, in fact, lower the risk of stroke,7 and that women with high cholesterol levels are at risk even if they are otherwise healthy.8 The American Heart Association now lists reducing the risk of stroke as the second most important reason for avoiding cholesterol-rich foods.3
Those who wish to believe in the association may be tempted to dismiss the old research as inferior by virtue of its comparative antiquity; those who wish to deny the association may be tempted to dismiss the new research as the product of an increasingly entrenched command of research dollars wielded by the manufacturers of cholesterol-lowering drugs. The truth lies somewhere between these two extremes.
Research over the last two decades has overcome many of the methodological flaws of earlier research and allowed us to recognize that cholesterol levels are indeed related to stroke—increasing the risk of some forms and decreasing the risk of others. Most important, this research has shown that oxidative stress, inflammation, and the health of the cells that line the blood vessel walls are the true causes underlying the efficacy of cholesterol-lowering statins. Careful examination of these findings allows us to assemble a strategy for preventing stroke within the context of a diet rich in traditional whole foods—including those rich in cholesterol.
Different Strokes
Although a given stroke may have more than one hundred potential causes, the vast majority of strokes fall roughly into two categories: hemorrhagic and ischemic. Hemorrhagic stroke occurs when a blood vessel ruptures, causing uncontrolled bleeding into brain tissue. Ischemic stroke occurs when a blockage closes off the flow of blood within a vessel, depriving brain tissue of the oxygen and nutrients it needs to survive. (In the US, over 90 percent of all strokes are ischemic.) The cell death that results from this deprivation is called an infarction. Severe buildup of atherosclerotic plaque can occasionally narrow a blood vessel sufficiently to produce an ischemic stroke, but it is usually a clot formed at the site of a ruptured plaque that causes such a stroke. Both forms of the disease cause lasting damage to the delicate tissue of the brain. Stroke is therefore not only the third leading cause of death but also the greatest single cause of disability in most developed countries.9
Finding the Correlation
In 1995, researchers pooled together the results of 45 prospective studies investigating the potential link between cholesterol levels and the risk of stroke. Together, these studies examined this relationship in 450,000 people. The risk of stroke declined slightly with increasing cholesterol levels—an effect so small that it could easily have been due to chance.5
Most studies that began in the 1960s and 1970s, before the advent of computed axial tomography (the CAT scan), failed to distinguish between ischemic and hemmhoragic strokes. Many of them were also primarily designed to study heart disease. Since strokes occur at a later age than heart attacks, the average age of the subjects in these studies was too young and the incidence of stroke too low to detect modest associations with risk factors. These two problems obscured the true relationship of cholesterol to stroke.10
The Honolulu Heart Study enrolled over 8,000 Japanese American men between 1965 and 1968, measured their cholesterol levels and recorded which of them died of stroke over the following six years. The men were between the ages of 45 and 68 at the time of enrollment. Although CAT scans were not yet available, the researchers distinguished between ischemic and hemorrhagic strokes using signs and symptoms, findings at surgery or autopsy. As published in a 1980 issue of the journal Stroke, they found no association between serum cholesterol and ischemic stroke and an inverse association between serum cholesterol and hemorrhagic stroke, meaning a higher cholesterol level was associated with a lower risk of hemorrhagic stroke.11
A second report from the Honolulu Heart Study, published in 1994 with a fifteen year follow-up, however, demonstrated a direct association between serum cholesterol and ischemic stroke. The association was only found among subjects with cholesterol levels higher than 213 milligrams per deciliter (mg/dL) and was very small—over the course of ten years, subjects with cholesterol levels under 213 had a 2.5 percent chance of stroke and those with levels over 240 had a 3.2 chance of stroke.12
This report also showed that the incidence of stroke increases with age to a much greater degree than does the incidence of heart disease. In men younger than sixty, the ratio of heart disease to stroke was greater than three; in men older than sixty, it was less than two.12 This pattern made the very meager association of ischemic stroke with serum cholesterol impossible to detect after only six years of follow-up.
The Multiple Risk Factor Intervention Trial (MR FIT) confirmed the findings of the Honolulu Heart Study in over 350,000 men. Those with cholesterol levels below 160 had three times the risk of hemorrhagic stroke as those with higher levels, while those with levels over 200 had a higher risk of ischemic stroke compared to those with lower levels. Between 200 and 240, the risk increased by only 20 percent. Those with levels above 280, however, had 2.5 times the risk of ischemic stroke as those with the lowest levels.13
The Eastern Stroke and Coronary Heart Disease Collaborative Research Group confirmed these findings in eastern Asian countries as well. The group pooled the results of 18 prospective studies conducted in China and Japan involving nearly 125,000 people. For every 23 point drop in serum cholesterol, the risk of ischemic stroke decreased by 23 percent and the risk of hemorrhagic stroke increased by 27 percent.14
It was then clear that the inability to discover a relationship of cholesterol levels to “stroke” resulted from the two opposing relationships of cholesterol levels to the two different types of stroke. The relationship between diet and stroke was less clear. Conventional wisdom would have had us believe that if high cholesterol levels increased the risk of ischemic stroke, so would a diet rich in total fat, saturated fat, and cholesterol. Conventional wisdom turned out to be very, very wrong.
A Greasy Situation
The authors of the 1980 Honolulu Heart Study report noted that stroke mortality and incidence among Japanese Americans was far lower than that among residents of Japan. They suggested that the difference owed to the substantially higher intakes of fat and protein among Japanese Americans.11 These authors published another report from the same study in 1985, which found an inverse association between ischemic stroke and the dietary intake of total and saturated fat.15
Other authors examined 198 autopsies of fatal stroke within the same study. They dissected small and large blood vessels of the brain and assessed the severity of atherosclerosis within them. Among 104 men who also had heart disease, there was no association between atherosclerosis and any dietary factors. Among the other 94, intake of fish was inversely associated with atherosclerosis of the small arteries and intake of animal protein and total fat was inversely associated with atherosclerosis of the large arteries. Intake of carbohydrates, by contrast, was positively associated with atherosclerosis of the large arteries.16
A decade later, the Framingham Heart Study found similar results among 800 men whom the researchers followed over the course of 19 years. Although there was no association of stroke with polyunsaturated fat consumption, each additional three percent of calories from total fat was associated with a fifteen percent decrease in the risk of ischemic stroke; each additional one percent of calories from monounsaturated fat was associated with an eleven percent decrease in risk; and each additional one percent of calories from saturated fat was associated with a nine percent decrease in risk.17
In the last decade, some studies have shown no relationship between the intake of animal fat and the risk of ischemic stroke, but most have continued to show that the risk of this disease is inversely associated with the intake of animal fat and fish.18
How Low Can it Go?
Early trials with cholesterol-lowering drugs were less than promising. A 1993 report pooled together the results of 13 trials conducted between 1966 and 1992 involving over 45,000 men. Cholesterol lowering had no effect on the incidence of stroke. There was a general tendency for it to decrease the risk of nonfatal stroke and increase the risk of fatal stroke, but the only trials in which the magnitudes of these differences were strong enough to be distinguished from the effects of chance were those that used the drug clofibrate. Clofibrate belongs to a class of drugs, called fibrates, that increase the excretion of lipids into the bile. Treatment with clofibrate more than doubled the risk of fatal stroke. The only trial that specifically reported the effect of treatment on hemorrhagic stroke used another fibrate called gemfibrozil. Treatment with this drug resulted in five times the risk of fatal hemorrhagic stroke.25
Hemorrhagic stroke is four times as deadly as ischemic stroke,21 and survival of both types is positively associated with cholesterol levels.22 The results of the early trials with cholesterol-lowering drugs may well reflect a tradeoff between hemorrhagic and ischemic stroke as well as a decreased ability to survive either type.
The results of later trials with statin drugs proved very different. A 2004 report that pooled together the results of 120 lipidlowering trials, including 24 using statins, showed that treatment with statins lowered the risk of stroke by 18 percent. Among ten trials that distinguished hemorrhagic from ischemic stroke, treatment with lipid-lowering therapy in general increased the risk of hemorrhagic stroke by 21 percent, whereas statins themselves increased this risk by only 3 percent; neither effect was large enough to be distinguished from the effect of chance.26 Statins are apparently more successful than older cholesterol-lowering drugs because they more effectively reduce the risk of ischemic stroke and less severely aggravate the risk of hemorrhagic stroke.
Some authors have suggested that statins effectively reduce the risk of stroke because they are more than twice as effective at reducing cholesterol levels compared to older drugs. Indeed, the older drugs only reduced cholesterol levels by an average of eight percent. Statins, by contrast, have reduced them by an average of 22 percent.27 Moreover, the reduction of LDL in these trials corresponds to both the reduction in the risk of stroke and the reduction in the degree of atherosclerosis within the arteries of the neck that supply the brain.28
If the key to the success of statins were limited simply to cholesterol reduction, however, we would expect them to not only lower the risk of ischemic stroke to a greater degree than other drugs, but also to raise the risk of hemorrhagic stroke to a greater degree than other drugs. Instead, we find that statins have no effect on the risk of hemorrhagic stroke at all. Clearly, these drugs are affecting the risk of stroke by some means other than lowering cholesterol.
Correlation versus Causation
It is a fundamental principle of science that correlation does not prove causation. The risk of ischemic stroke is higher among people with high cholesterol levels, but this does not in and of itself show that high cholesterol levels cause ischemic stroke. If a drug that lowers cholesterol also lowers the risk of this disease and the reduction in risk is proportionate to the reduction in cholesterol, this provides evidence that high cholesterol causes the disease—as long as the drug only lowers cholesterol. With statins, however, this is not the case.
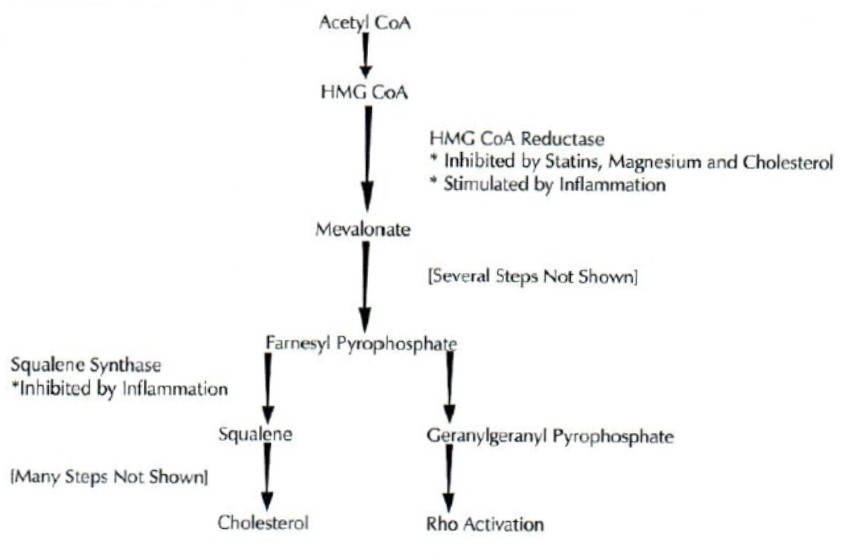
Statins do not directly inhibit the synthesis of cholesterol. Instead, they inhibit the synthesis of mevalonate (see Figure 1). Cells use mevalonate to synthesize a number of different chemicals, only one of which is cholesterol. The degree of cholesterol reduction is dependent on the degree of mevalonate reduction; it therefore can also act as a marker for the degree of reduction of other products made from mevalonate. Before concluding which of these products underlies the efficacy of statins, we must look beyond statistical correlations and examine more deeply the molecular mechanisms of the disease process.
Figure 1. Cholesterol Synthesis and Rho Activation
Many steps in the cholesterol synthesis pathway are omitted in the figure for the sake of simplicity. The key regulated enzymes within this pathway are HMG CoA reductase and squalene synthase. The former converts HMG CoA to mevalonate; the latter converts farnesyl pyrophosphate to squalene. The synthesis of squalene is the first step in this pathway that is committed to the synthesis of cholesterol. Statins suppress both the synthesis of cholesterol and the activation of Rho by inhibiting HMG CoA reductase. Inflammation increases cholesterol levels by stimulating HMG CoA reductase; because it also inhibits squalene synthase, however, most of the mevalonate it produces is diverted into other pathways, such as Rho activation. Because they inhibit HMG CoA reductase, it is possible that magnesium and dietary cholesterol also suppress Rho activation.
Nitric Oxide
One of the many products of mevalonate activates the enzyme Rho. Rho is a stress signal which, in response to inflammation, changes the shape and tension of the protein fibers that form the cell’s skeleton.29 Rho also decreases the production of endothelial nitric oxide synthase (eNOS), the enzyme that synthesizes nitric oxide.30 Nitric oxide itself is a gas that dilates blood vessels, relaxing the smooth muscle cells within their walls and increasing the flow of blood. It also decreases the adhesion of white blood cells to the lining of these vessels, the migration of smooth muscle cells to the sites of atherosclerotic lesions and the formation of blood clots, all of which are involved in the disease process that leads to ischemic stroke.31
By inhibiting the activation of Rho,30 statins greatly increase the levels of eNOS and the amount and activity of nitric oxide within the blood vessel lining.32,33 When researchers experimentally induce a stroke in mice with normal cholesterol levels, prior administration of statins greatly increases the flow of blood within the brain and reduces the damage to brain tissue and the neurological deficits that follow. The benefit occurs even when the dose and length of administration is insufficient to reduce cholesterol; in mice that are genetically engineered to lack the eNOS enzyme, by contrast, statins have no effect.34 These drugs clearly protect against stroke in ways that are dependent on eNOS and have nothing to do with cholesterol.
There is also evidence that the inhibition of Rho offers additional protection against stroke in some animal models by increasing the body’s ability to dissolve blood clots independently of both eNOS and cholesterol.35
Because both Rho activation and cholesterol synthesis depend on the availability of mevalonate, the ability of a given drug or a given dose of that drug to inhibit one substance is going to correlate with its ability to inhibit the other. These things make it clear that a protective effect of statins—even one that correlates with cholesterol reduction—is not necessarily evidence that cholesterol itself causes stroke.
Is Cholesterol Irrelevant?
It would be a mistake to conclude from these observations that cholesterol is entirely irrelevant to the process that leads to ischemic stroke. Most likely, the level of low-density lipoprotein (LDL) cholesterol is a loose indicator of the level of oxidized LDL, a particle that can, indeed, contribute to the disease process that underlies this form of stroke.
An LDL particle carries cholesterol and triglycerides through the blood within a membrane made of lipid and protein. The membrane consists primarily of many phospholipids interwoven with one large protein molecule; although most of the cholesterol is contained within the core of the particle, a small amount is also distributed throughout the membrane. The amino acids within the protein and the unsaturated fatty acids within the phospholipids are vulnerable to oxidation; they are also protected by certain vitamins, polyphenols and other antioxidants that are carried within the lipoprotein. When we refer to the oxidation of LDL, we refer primarily to the oxidation of the phospholipids and protein at the surface of the particle rather than the cholesterol within its core.
Oxidation of LDL causes it to accumulate in certain scavenger white blood cells called macrophages—an instrumental event in its accumulation within atherosclerotic plaque.41 Oxidized LDL also suppresses the production of eNOS. Since nitric oxide inhibits the oxidation of LDL, the loss of nitric oxide and the oxidation of LDL could produce a vicious cycle.33 When the level of sugar in the blood rises, it can similarly damage LDL in a process called glycation. Although less powerfully than oxidized LDL, glycated LDL also accumulates in macrophages42 and suppresses the production of eNOS.43
Selectively filtering LDL from the blood of patients with high cholesterol—most of which is oxidized—appears to improve nitric oxide production and blood flow.44 Researchers have unfortunately only tested the effect of this treatment on these parameters in small, uncontrolled trials.
We cannot with any confidence quantify the contribution of oxidized LDL to the development of stroke, but the evidence strongly suggests that it plays some part. The very meager association between cholesterol levels and ischemic stroke probably reflects both the indirect association of cholesterol with chronic inflammation (see sidebar) and the causal contribution of oxidized LDL.
Low Cholesterol and Hemorrhagic Stroke
Whether and how low cholesterol causes the increased risk of hemorrhagic stroke with which it is associated is an open question. Animal experiments have shown that diets high in animal fat and cholesterol reduce the incidence of stroke in rats with high blood pressure.17 In humans, the inverse association between cholesterol levels and hemorrhagic stroke primarily exists among those with diastolic blood pressure above 90 millimeters mercury (mm Hg).13 Cholesterol probably protects against hemorrhage by strengthening and stabilizing the blood vessel walls, especially when these walls need extra strength to withstand the constant onslaught of high blood pressure.
Practical Prevention
Despite the opposing relationships of cholesterol levels to ischemic and hemorrhagic strokes, the distribution of risk is not even across cholesterol levels. In the large MR FIT trial, for example, stroke mortality was lowest between 180 and 200. Mortality substantially increased below 180 and above 240; it was highest below 160 and above 300.13 While it is unlikely that total or LDL cholesterol themselves play a major role in the development of stroke, oxidation or glycation of that LDL will contribute to the atherosclerotic process and the breakdown of nitric oxide functioning. It therefore may be a sensible precaution to use exercise and, where needed, nutritional supplements to maintain moderate levels of cholesterol and to eat a diet rich in antioxidants to protect that cholesterol from damage.
Magnesium is essential to the regulation of cholesterol synthesis. Like statin drugs, magnesium inhibits the enzyme that produces mevalonate, a precursor to cholesterol. Unlike statins, however, cellular enzymes also use magnesium to increase the production of mevalonate when needed. Supplements with this mineral can lower levels of LDL and raise levels of HDL; since they provide the body with the resources it needs to regulate these levels rather than interfere with the body’s physiological processes, they are unlikely to exhibit any of the adverse effects exhibited by statins.39
Diets low in fat or animal products should not be used to lower cholesterol for the prevention of ischemic stroke. The available data clearly indicate that these foods are associated with a decreased risk, not an increased risk, of this type of stroke.17 Since carbohydrate intake is associated with atherosclerosis of the large arteries within the brain,16 eating lower amounts of carbohydrates would be a wiser dietary modification.
Additionally, increasing polyunsaturated fat intake in the DART trial doubled stroke mortality.23 Polyunsaturated fatty acids are vulnerable to oxidation within the body49 and their incorporation into lipoproteins would make those lipoproteins more likely to oxidize. Since there is evidence that fatty fish is protective against stroke,18 however, we should give priority to reducing omega-6 fatty acids from vegetable oils rather than the elongated omega-3 fatty acids from fish. Even among traditional fats, an overemphasis on olive oil, flax oil, chicken fat, or even very large amounts of lard could lead us to consume an excess of polyunsaturated fat. These nourishing foods have their place, but more saturated fats like butter, tallow and coconut oil should form the mainstay of a diet rich in fat.
Exercise, antioxidant-rich foods and proper treatment of chronic oral or systemic infections will help maintain the rich supply of nitric oxide that blood vessels need. Since the amino acid L-arginine is the raw material for nitric oxide production, adequate protein is also important.
Blood pressure is far more critical to the development of stroke than is cholesterol. Exercise, stress management and adequate intake of potassium can be useful in controlling blood pressure. Some individuals may also need to moderate their intake of salt.
Were it true, as many contend, that the consumption of cholesterol-rich animal foods such as butter, egg yolks and organ meats puts one at risk for stroke, we would be forced to make the difficult choice between the diet that builds robust and sturdy bodies and the diet that allows us to live safely into old age. Thankfully, there is no evidence that these foods will do anything but protect us from stroke. Nutrient-dense animal foods are gifts for which we should all be grateful. They supply the body with the resources it needs both to build itself up during youth and to maintain its integrity into old age.
Sidebars
A Question of Bias
A case control study of 180 subjects published in 1996 showed that LDL-cholesterol had a strong, positive association with ischemic stroke and that HDL-cholesterol had a strong, negative association with ischemic stroke. The authors were surprised to find, however, that saturated fat intake was over 25 percent lower in stroke patients than in controls.19
Case control studies are conducted retrospectively—that is, after the endpoints or results one is trying to learn about have already occurred. For this reason, they are subject to a number of biases to which prospective studies are not. The authors of this report suggested that the inverse association of stroke with the intake of saturated fat resulted from one of these biases: patients who have a history of high cholesterol and triglycerides would be counseled to avoid saturated fat. Therefore, they argued, the low intake of saturated fat would not have caused the disease; rather, the disease would have caused the low intake of saturated fat.
To support this proposition, they examined the medical records of a subset of their subjects to see whether a prior diagnosis of high lipid levels was associated with a low intake of saturated fat during the time of the study. Indeed, this was the case. They produced no evidence, however, that the diet followed rather than preceded the diagnosis. If it is true that the patients only followed a low-fat diet after being diagnosed with high lipid levels, it leaves open the question of why the diet did not lower their lipid levels or their risk of stroke. The suggestion that the low intake of saturated fat was caused by the disease rather than the disease by the low intake of saturated fat may have been easier to reconcile with the researchers’ presuppositions, but it is more difficult to reconcile with the consistent evidence from prospective studies that total fat and animal fat consumption is inversely associated with the incidence of stroke.
Take Your Pick
In his book Eat to Live, Dr. Joel Fuhrman argues that avoiding animal foods is an important strategy for stroke prevention. Although low cholesterol levels increase the risk of hemorrhagic stroke, this type only represents eight percent of the total; since the vast majority of strokes are of ischemic origin, he maintains, eating a cholesterol-lowering diet will lower the risk of stroke.20
This point of view suffers from three fundamental flaws: first, the data indicates that the rate of hemorrhagic stroke is low in western countries because our cholesterol levels tend to be high; second, hemorrhagic strokes are far more dangerous than ischemic strokes; and third, as already shown, animal foods are associated with a decrease—not an increase—in the risk of ischemic stroke.
Among Japanese American men living in Hawaii, whose intakes of animal fat and protein are lower than those of mainland Americans but higher than those of men living in Japan, hemorrhagic stroke constitutes 25 percent of all strokes.11 In China and Japan, where serum cholesterol levels correspond to the bottom two thirds of the range of western levels, hemorrhagic stroke constitutes 42 percent of all strokes. The authors of a collaborative research project pooling the results of 18 studies conducted in this region found that as cholesterol levels increased, hemorrhagic stroke constituted a lower proportion of total strokes; as cholesterol levels decreased, hemorrhagic stroke constituted a higher proportion of total strokes.14 Although the risk of hemorrhagic stroke may be low in the United States, the rates of this more dangerous type of stroke would almost certainly be higher if we vigorously maintained low cholesterol levels by eating vegan or semi-vegan diets.
Hemorrhagic stroke is much more dangerous than ischemic stroke. Victims of the former suffer greater neurological deficits, are more likely to be institutionalized, and are four times more likely to die within thirty days than victims of the latter. A recent comparison of the two types showed that only seven percent of ischemic stroke victims die within thirty days, whereas 28 percent of hemorrhagic stroke victims die within the same period of time.21 Moreover, low cholesterol levels are associated with decreased survival even from ischemic stroke. A Scottish study found that every 40 point decrease in serum cholesterol was associated with a nine percent increase in the risk of mortality for all types of stroke.22
In the MR FIT trial, involving over 350,000 men, stroke mortality was lowest among those with cholesterol levels between 180 and 200. Substantial increases in mortality occurred below 180 and above 240. The largest increases in mortality occurred among those with levels below 160 and over 300.13 Although these correlations do not demonstrate that the cholesterol levels actually cause the increase or decrease in risk, in the absence of a comprehensive understanding of causation they may justify optimizing these levels with exercise, nutritional supplements or moderation of carbohydrate intake. They cannot, however, justify a diet low in animal protein and fat when the evidence has consistently shown the consumption of these foods to be associated with an equal or lower risk of stroke.
In the Diet and Reinfarction Trial (DART), subjects who reduced their total fat intake and replaced saturated fat with polyunsaturated fat doubled their risk of suffering a fatal stroke.23 The reduction of total fat was small, from 35 percent of calories to 32 percent of calories. The increase in the polyunsaturated-to-saturated fat ratio was larger: it doubled from 0.4 to 0.8. These results taken together suggest that maintaining low cholesterol levels with diets low in fat and saturated fat is likely to increase the risk and severity of stroke.
A Convenient Choice of Words
On February 20, 2007, Science Daily reported that researchers had shown total cholesterol levels to predict the risk of stroke in women. Women with the highest cholesterol levels, according to the article, had twice the risk of stroke as women with lower levels. The researchers claimed their findings underscored “the importance of cholesterol levels as a risk factor for stroke, even if you have no history of heart disease and are otherwise healthy.”8
The article left out one important fact: the study only looked at ischemic stroke.24 Did the women with high cholesterol levels have not only twice the risk of ischemic stroke but also half the risk of the much more dangerous and fatal hemorrhagic stroke? Was the incidence of total stroke any higher or lower in women with high cholesterol levels? We simply do not know; the study did not address the question.
Chronic Nitric Oxide Deficiency
Many dietary, lifestyle, and physiological factors directly or indirectly regulate nitric oxide levels. Nitric oxide relaxes blood vessels, increases blood flow and inhibits the formation of atherosclerotic plaque. A chronic deficiency of this compound may be among the most important causes of atherosclerosis and ischemic stroke.
The enzyme endothelial nitric oxide synthase (eNOS) produces nitric oxide within the lining of the blood vessels. Many factors regulate the production of this enzyme and thereby indirectly regulate the production of nitric oxide itself. Sheer stress stimulates the production of eNOS and may be an important mediator of the atherosclerotic process. The blood vessel lining experiences this type of stress as blood runs parallel to it. Exercise increases sheer stress because it causes the blood to move more vigorously, and thereby increases the production of eNOS.36 Atherosclerotic lesions tend to develop at specific sites where disturbed blood flow increases the force running perpendicular to the blood vessel lining and decreases the force running parallel to it.37
Oxidized LDL-cholesterol and insufficient oxygen decrease the production of eNOS. Free radicals are able to destroy nitric oxide itself after eNOS has synthesized it.38
The cellular enzyme Rho is capable of powerfully suppressing the production of eNOS. Ordinarily, the vast majority of Rho within a cell is inactivated. One of the products of the cholesterol synthesis pathway, geranylgeranyl pyrophosphate (GGPP), is responsible for activating it. Cellular enzymes synthesize GGPP from mevalonate. When the cell is producing more mevalonate than it uses for cholesterol synthesis, more GGPP is available for the activation of Rho (see Figure 1). Dietary nutrients such as cholesterol and magnesium, as well as the cholesterol that we synthesize ourselves, keep the production of mevalonate from exceeding the level needed by the cell.39 Inflammation, however, not only increases the production of mevalonate but inhibits its conversion to cholesterol. When researchers fed hamsters endotoxin, a proinflammatory chemical released from the breakdown of bacterial cell walls, it increased the production of mevalonate by a factor of ten but only increased the production of cholesterol by a factor of two.40 The result of chronic inflammation is a small excess of cholesterol and a much larger excess of other mevalonate products such as GGPP, which our cells then use to activate Rho.
Magnesium deficiency, chronic inflammation—and perhaps even a lack of dietary cholesterol—might contribute to chronic activation of Rho and suppression of nitric oxide synthesis. Inadequate exercise, excessive consumption of easily oxidized materials such as polyunsaturated fat and inadequate dietary antioxidants may further aggravate the deficiency of this important compound and thereby facilitate the atherosclerotic process and the impairment of blood flow that characterize an ischemic stroke.
Blood Pressure and Stroke
The overwhelmingly powerful and consistent risk factor for stroke is not high cholesterol but high blood pressure.
The 1980 report of the Honolulu Heart Study found the risk of ischemic stroke to increase with systolic blood pressure beginning at the lowest levels—the risk was lowest at levels under 121 millimeters mercury (mm Hg). The relationship of blood pressure to hemorrhagic stroke was similar but the lowest risk existed at levels between 122 and 134 mm Hg. The authors concluded that, “It seems to be a universal finding among all stroke epidemiology studies that the single most important risk factor for stroke, whether of cerebral infarction or intracranial hemorrhage, is hypertension.”15
In a 1995 report of the pooled results of 45 prospective studies involving 450,000 people, the risk of stroke had no association with cholesterol, but it increased consistently with diastolic blood pressure from the group with the lowest to the group with the highest. The difference was dramatic: subjects with a diastolic blood pressure of 102 mm Hg had five times the risk of stroke as those with a diastolic blood pressure of 75 mm Hg.5
In a 1998 report of the pooled results of 18 prospective studies conducted in eastern Asia involving nearly 125,000 people, the effect of blood pressure was even more pronounced. While serum cholesterol had modest but opposing associations with ischemic and hemorrhagic strokes that canceled each other out, the risk of both types of stroke increased consistently as diastolic blood pressure increased. Those with levels higher than 110 mm Hg had 13 times the risk of stroke as those with levels lower than 79 mm Hg.14
Clearly, maintaining optimal blood pressure is far more important to preventing stroke than maintaining low cholesterol levels.
The Work Of Weston Price: Its Enduring Value
Weston Price promoted two theories about the relationship of nutrition and oral health to degenerative disease, which have long been ignored but have more recently gained support. In his earlier career, Price conducted 25 years of research demonstrating the ability of oral pathogens to cause cardiovascular and other systemic diseases. His work focused primarily on the tendency of the root canal procedure to facilitate this process.45 In his classic work on nutrition, Nutrition and Physical Degeneration, he connected nutritional status during development to deformities of the oral palate as well as to the risk of tuberculosis. Price believed that developmental deformities of the chest cavity—produced by the same nutritional causes as the deformities of the oral palate—made a person more vulnerable to the tuberculosis bacterium. For these reasons, he placed a special emphasis on the importance of nutritional preparation for and support of pregnancy and lactation—practices he universally observed among the healthy indigenous groups he studied.2 Modern science is now rediscovering the links between vascular disease and oral health and fetal nutrition.
Oral Health and Stroke
Recent research has been focusing on the association of vascular disease with periodontitis rather than with root canals, but nevertheless has been confirming the general principle observed by Price, namely that oral pathogens can cause systemic, degenerative diseases. Oral pathogens and immune cells specific to them inhabit arterial plaque. A number of studies have associated periodontitis with the severity of atherosclerosis and the incidence of heart disease and stroke. The pooled results of these studies conducted up to the year 2004 associate the presence of periodontitis with a 50 percent increase in the risk of ischemic stroke. Several studies have associated the presence of severe periodontitis with a nearly three-fold increase in risk of total stroke or fatal ischemic stroke. Among those strokes that are preceded by a fever, dental infection is associated with a nine-fold increase in risk.46
Preliminary evidence suggests that periodontitis increases the systemic marker of inflammation known as C-reactive protein as well as total and LDL-cholesterol. Intensive treatment of periodontitis using antibiotics decreases these levels when compared to standard treatment without antibiotics.47 Although it is possible that LDL and total cholesterol may be an important part of the body’s response to inflammation, it is also possible that their increase is largely coincident with the increase in mevalonate production used for other purposes, such as the activation of Rho, an important mediator of the stress response (see sidebar).
Oral pathogens may cause immune cells specific to them to directly adhere to the blood vessel lining and initiate atherosclerosis. By increasing the activation of Rho, however, we should also expect systemic inflammation to interfere with nitric oxide functioning and thereby contribute to atherosclerosis by a second mechanism.
Fetal Nutrition and Stroke
Recent research has focused on the association of fetal nutrition with certain physical deformities and the risk of vascular diseases rather than the risk of tuberculosis; nevertheless, this research confirms the general principle that early nutritional status has a lasting influence on the risk of degenerative disease. Inadequate nutrition during various stages of fetal development causes corresponding changes in various physical parameters; these parameters are in turn associated with the risk of diabetes, heart disease and stroke.
Soon after conception, inadequate nutrition causes the womb to reallocate cells from the fetus to the placenta in order to extract more nutrition from the blood supply of the mother; the inevitable result is a loss of raw material from which to generate fetal tissue. During later stages of growth, the fetus compensates for inadequate nutrition by sacrificing the supply of nutrients to muscles and internal organs such as the liver and pancreas in favor of supplying the brain; the exception is the left ventricle of the heart, which may grow larger than is normal in order to pump hard enough to supply the brain with extra blood. This general pattern of compensation results in a reduced ratio of body length to head circumference (that is, short stature with a proportionately larger head).48
Excluding premature births, low birth weight is associated with a three-fold increase in the risk of type-2 diabetes, a two-fold increase in the risk of heart disease and a modest increase in life-long blood pressure. A reduced length-to-head circumference ratio is associated with defects in the regulation of cholesterol and blood clotting metabolism. One study found stroke mortality to be more common among men who were born to mothers with flat, bony pelvises (considered abnormal), suggesting a relationship between the mother’s childhood nutrition and her offspring’s risk of stroke.48
These findings illustrate the enduring importance of Price’s research and the benefits that would accrue should modern science incorporate his research into the paradigm with which it approaches questions of health and disease.
REFERENCES
- Masterjohn C. The Many Functions of Cholesterol. http://www.cholesterol-and-health.com/Functions-Of-Cholesterol.html. Published 2005. Accessed August 18, 2007.
- Price W. Nutrition and Physical Degeneration: 6th Edition. La Mesa, CA: Price-Pottenger Nutrition Foundation. 2004.
- American Heart Association. How Can I Lower High Cholesterol? http://www.americanheart.org/downloadable/heart/110288182952015LwrHighChol.pdf. Published 2004. Accessed August 18, 2007.
- Heron MP, Smith BL. Deaths: leading causes for 2003. Natl Vital Stat Rep. 2007;55(10):1-92.
- Prospective Studies Collaboration. Cholesterol, diastolic blood pressure, and stroke: 13,000 strokes in 450,000 people in 45 prospective cohorts. Lancet 1995;346:1647-53.
- Atkins D, Psaty BM, Koepsell TD, Longstreth WT, Larson EB. Cholesterol Reduction and the Risk for Stroke in Men. Ann Intern Med. 1993;119(2):136-45.
- Science Daily. Cholesterol-lowering Drugs Reduce Risk of Stroke, Heart Attack. http://www.sciencedaily.com/releases/2007/05/070502172322.htm. Published May 8, 2007. Accessed August 18, 2007.
- Science Daily. Healthy Women With High Cholesterol At Increased Risk of Stroke. http://www.sciencedaily.com/releases/2007/02/070220020827.htm. Published February 20, 2007. Accessed August 18, 2007.
- Collins C. Pathophysiology and classification of stroke. Nurs Stand. 2007;21(28):35-39.
- Demchuk AM, Hess DC, Brass LM, Yatsu FM. Is Cholesterol a Risk Factor for Stroke? Yes. Arch Neurol. 1999;56(12):1518-20.
- Kagan A, Popper JS, Rhoads GG. Factors related to stroke incidence in Hawaii Japanese men. The Honolulu Heart Study. Stroke. 1980;11:14-21.
- Benfante R, Yano K, Hwang L-J, Curb JD, Kagan A, Ross W. Elevated Serum Cholesterol Is a Risk Factor for Both Coronary Heart Disease and Thromboembolic Stroke in Hawaiian Japanese Men. Implications of Shared Risk. Stroke. 1994;25:814-820.
- Iso H, Jacobs Jr. DR, Wentworth D, Neaton JD, Cohen JD for the MRFIT Research Group. Serum cholesterol levels and six-year mortality from stroke in 350,977 men screened for the multiple risk factor intervention trial. New Engl J Med. 1989;320:904-10.
- Eastern Stroke and Coronary Heart Disease Collaborative Research Group. Blood pressure, cholesterol, and stroke in eastern Asia. Lancet. 1998;352:1801-07.
- Kagan A, Popper JS, Rhoads GG, Yano K. Dietary and other risk factors for stroke in Hawaiian Japanese men. Stroke. 1985;16:390-396.
- Reed DM, Resch JA, Hayashi T, MacLean C, Yano K. A prospective study of cerebral artery atherosclerosis. Stroke. 1988;19:820-825.
- Gillman MW, Cupples A, Millen BE, Ellison RC, Wolf PA. Inverse Association of Dietary Fat With Development of Ischemic Stroke in Men. JAMA. 1997;278:2145-2150.
- He K, Xu Y, Van Horn L. The Puzzle of Dietary Fat Intake and Risk of Ischemic Stroke: A Brief Review of Epidemiologic Data. J Am Diet Assoc. 2007;107:287-295.
- Hachinski V, Graffagnino C, Beaudry M, Bernier G, Buck C, Donner A, Spence D, Doig G, Wolfe BMJ. Lipids and Stroke: A Paradox Resolved. Arch Neurol. 1996;53:303-308.
- Fuhrman J. Eat to Live: The Revolutionary Formula for Fast and Sustained Weight Loss. New York, NY: Little, Brown and Company. 2003; pp.132-133.
- Barber M, Roditi G, Stott DJ, Langhorne P. Poor outcome in primary intracerebral haemorrhage: results of a matched comparison. Postgrad Med J. 2004;80:89-92.
- Dyker AG, Weir CJ, Lees KR. Influence of cholesterol on survival after stroke: a retrospective study. BMJ. 1997;314:1584.
- Ness AR, Hughes J, Elwood PC, Whitley E, Smith GD, Burr ML. The long-term effect of dietary advice in men with coronary disease: follow-up of the Diet and Reinfarction trial (DART). Eur J Clin Nutr. 2002;56:512-518.
- Kurth T, Everett BM, Buring JE, Kase CS, Ridker PM, Gaziano JM. Lipid levels and the risk of ischemic stroke in women. Neurology. 2007;68(8):556-62.
- Atkins D, Psaty BM, Koepsell TD, Longstreth WT, Larson EB. Cholesterol Reduction and the Risk for Stroke in Men. A Meta-Analysis of Randomized, Controlled Trials. Ann Intern Med. 1993;119(2):136-145.
- Briel M, Studer M, Glass TR, Bucher HC. Effects of Statins on Stroke Prevention in Patients with and without Coronary Heart Disease: A Meta-analysis of Randomized Controlled Trials. Am J Med. 2004; 117:596-606.
- Corvol J-C, Bouzamondo A, Sirol M, Hulot J-S, Sanchez P, Lechat P. Differential Effects of Lipid-Lowering Therapies on Stroke Prevention. A Meta-analysis of Randomized Trials. Arch Intern Med. 2003; 163:669-676.
- Amarenco P, Labreuche J, Lavallée, Touboul P-J. Statins in Stroke Prevention and Carotid Atherosclerosis: Systematic Review and Up-to-Date Meta-Analysis. Stroke. 2004;35:2902-2909.
- Wojciak-Stothard B, Ridley AJ. Rho GTPases and the regulation of endothelial permeability. Vasc Pharmacol. 2003;39:187-199.
- Laufs U, Liao JK. Post-transcriptional Regulation of Endothelial Nitric Oxide Synthase mRNA Stability by Rho GTPase. J Biol Chem. 1998;273(37):24266-24271.
- Miida T, Takahashi A, Ikeuchi T. Prevention of stroke and dementia by statin therapy: Experimental and clinical evidence of their pleiotropic effects. Pharmacol Ther. 1007;113:378-393.
- Laufs U, Fata VL, Liao JK. Inhibition of 3-Hydroxy-3-methylglutaryl (HMG)-CoA Reductase Blocks Hypoxiamediated Down-regulation of endothelial Nitric Oxide Synthase. J Biol Chem. 1997;272(50):31725-31729.
- Laufs U, Fata VL, Plutzky J, Liao JK. Upregulation of Endotelial Nitric Oxide Synthase by HMG CoA Reductase Inhibitors. Circulation. 1998;97:1129-1135.
- Endres M, Laufs U, Huang Z, Nakamura T, Huang P, Moskowitz MA, Liao JK. Stroke protection by 3-hydroxy-3- methylglutaryl (HMG) CoA reductase inhibitors mediated by endothelial nitric oxide synthase. Proc Natl Acad Sci USA. 1998;95:8880-8885.
- Asahi M, Huang Z, Thomas S, Yoshimura S, Sumii T, Mori T. Protective effects of statins involving both eNOS and tPA in focal cerebral ischemia. J Cereb Blood Flow Metab. 2005;25(6):722-9.
- Searles CD. Transcriptional and posttranscriptional regulation of endothelial nitric oxide synthase expression. Am J Physiol Cell Physiol. 2006;291:803-816.
- Libby P. Inflammation and cardiovascular disease mechanisms. Am J Clin Nutr. 2006;83(Suppl):456S-60S.
- Mason RP. Molecular Basis of Differences Among Statins and a Comparison with Antioxidant Vitamins. Am J Cardiol. 2006;98[suppl]:34P-41P.
- Rosanoff A, Seelig MS. Comparison of Mechanism and Functional Effects of Magnesium and Statin Pharmaceuticals. J Am Coll Nutr. 2004;23(5):501S-505S.
- Memon RA, Shechter I, Moser AH, Shigenaga JK, Grunfeld C, Feingold KR. Endotoxin, tumor necrosis factor, and interleukin-1 decrease hepatic squalene synthase activity, protein, and mRNA levels in Syrian hamsters. J Lipid Res. 1997;38:1620-1629.
- Prescott MF, Muller KR, Flammer R, Feige U. The effect of LDL and modified LDL on macrophage secretion products. Agents Actions Suppl. 1994;16:163-70.
- Rashid I, van Reyk DM, Davies MJ. Carnosine and its constituents inhibit glycation of low-density lipoproteins that promotes foam cell formation in vitro. FEBS Letters. 2007;581:1067-1070.
- Ji Y, Diao J, Han Y, Huang Y, Bai H, Chen Q, Leming F, Ferro A. Pyridoxine prevents dysfunction of endothelial cell nitric oxide production in response to low-density lipoprotein. Atherosclerosis. 2006;188:84-94.
- Tamai O, Matsuoka H, Itabe H, Wada Y, Kohno K, Imaizumi T. Single LDL Apheresis Improves Endothelium-Dependent Vasodilatation in Hypercholesterolemic Humans. Circulation. 1997;95:76-82.
- Meinig GE. Root Canal Cover-Up: A Founder of the Association of Root Canal Specialists Discovers Evidence That Root Canals Damage Your Health: Learn What to Do. Ojai, CA: Bion Publishing. 1998.
- Meurman JH, Sanz M, Janket S-J. Oral Health, Atherosclerosis, and Cardiovascular Disease. Crit Rev Oral Biol Med. 2004;15(6):403-413.
- D’Aiuto F, Nibali L, Parkar M, Suvan J, Tonetti MS. Short-term Effects of Intensive Periodontal Therapy on Serum Inflammatory Markers and Cholesterol. J Dent Res. 2005;84(3):269-273.
- Barker DJP. Fetal nutrition and cardiovascular disease in later life. Brit Med Bull. 1997;53(1):96-108.
- Saito M, Kubo K. Relationship between tissue lipid peroxidation and peroxidizability index after alpha-linolenic, eicosapentaenoic, or docosahexaenoic acid intake in rats. Br J Nutr. 2003;89(1:19-28.
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly magazine of the Weston A. Price Foundation, Fall 2007.
🖨️ Print post
Thank you Chris Masterjohn
This article is a gold mine of information for one looking at the atherosclerosis puzzle from many angles. You have filled in several “Terra Incognita” for me.
Your observation that
“Magnesium deficiency, chronic inflammation—and perhaps even a lack of dietary cholesterol—might contribute to chronic activation of Rho and suppression of nitric oxide synthesis. Inadequate exercise, excessive consumption of easily oxidized materials such as polyunsaturated fat and inadequate dietary antioxidants may further aggravate the deficiency of this important compound and thereby facilitate the atherosclerotic process and the impairment of blood flow that characterize an ischemic stroke.”
Is about as close to a succinct golden rule for sound cardiovascular health as we are likely to see.
IMO you should be able to get your PhD while asleep. Doctor Otto Warburg made perhaps the greatest discovery in medicine as a chemist. Lets see what a history major can do. LOL!
Check this paragraph please
QUOTE:
[b}”Diets LOW IN FAT or ANIMAL PRODUCTS should NOT be used to lower cholesterol for the prevention of ischemic stroke. The available data clearly indicate that THESE FOODS are associated with a DECREASED risk, not an increased risk, of this type of stroke.17 Since carbohydrate intake is associated with atherosclerosis of the large arteries within the brain,16 eating lower amounts of carbohydrates would be a wiser dietary modification.”
Great article!!
However I wonder whether there is a typo in the above paragraph – which seems to contain double negatives – should this not in fact be recommending higher-fat diets? The way it is written, suggests that although low-fat foods lower cholesterol AND decrease stroke risk, they should not be used, which seems antithetical to the article’s intent.
Check this paragraph please
LRJ, you are reading the sentence wrong. It says “The available data clearly indicate that THESE FOODS [FAT or ANIMAL PRODUCTS] are associated with a DECREASED risk”
It is confusing, I’ll admit, as I had to read it twice to get the real meaning.
This was written in 2009. It is 2015. Any new research that affirms or contradicts the findings published in 2009?
Interesting article. If this information is true, we would expect to see an significant increase in hemorrhagic stroke in the vegan population, since cholesterol levels are typically much lower than 180 in people maintaining this kind of diet. Do you have any research that demonstrates this? Do you have any clinical research that demonstrates disease states more frequently experienced by vegans compared to omnivores or those following a paleo diet?