






Addressing Thyroid and Adrenal Insufficiency
Are you often tired or worn down? Do you have trouble sleeping? Do you have problems with your weight? Do you feel as though you’re cold all the time and can’t warm up? Do you have dry skin? Do you sometimes have difficulty remembering things? If the answer is “yes” to any of the above and you’re thinking it’s just something you have to live with, think again.
While all of the above seem like nothing more than day-to-day annoyances, in reality all are symptoms of low metabolic energy. The best way to eliminate these symptoms—and restore metabolic energy—is to correct the underlying problem. What causes low metabolic energy? The most common cause is poor thyroid function, poor adrenal function or, most commonly, a mixture of both. Another very frequent cause is hormonal imbalance— especially low progesterone or estrogen dominance in women or low testosterone in men. Restoring metabolic energy helps the body help itself, letting the self-repair mechanisms function well again and restore health.
What Causes Low Metabolic Energy?
Every process that goes on inside our bodies requires energy – specifically metabolic energy. When the body doesn’t have enough energy to function properly, each component of the body will malfunction in its own unique way. For example, if the brain has too little energy, thought processes such as memory and focus become impaired.
The body needs energy to keep itself warm; a low body temperature, therefore, usually accompanies low metabolic energy. (For more examples see the symptoms list, page 17.) In our cells, ready-to-use energy is present in the form of ATP (adenosine triphosphate) molecules. The body converts fats and carbohydrates into ATP that is then used for energy. However, there are other factors involved that can affect how well our body can make this conversion.
The thyroid gland, located at the base of the neck, make the hormone T4 (thyroxine). T4 converts to T3 (triiodothryronine) and RT3 (reverse T3). It is T3 that turns on the ATP-making machinery inside each living cell, while the RT3 slows it down. Production of these thyroid hormones is controlled by TSH (thyroid stimulating hormone), which is released by the pituitary gland in the brain. The pituitary takes its orders from the hypothalamus (also part of the brain).
The adrenal glands, located on top of each kidney, help the body deal with stress. If metabolic activity is excessive, the adrenals perceive this as a stress. In response to this stress, the hypothalamus will signal the pituitary to produce less TSH, thus producing decreased T4 and thyroid activity. Based on the above explanation, some of the contributors to low metabolic energy are as follows:
- The thyroid gland cannot make enough T4 (hypothyroidism).
- The adrenal glands are too weak to handle the stress of the body’s normal metabolic energy and force a down-regulation of energy production.
- The enzymes (cellular machinery) which make ATP may be held back due to chemical interference from toxins, lack of needed ingredients (vitamins or minerals), or breakdown due to auto-immune disease or old viral damage.
- Imbalance of hormones, such as growth hormone, testosterone, estrogen or progesterone.
- Severe caloric restriction.
When one or a combination of these factors is in place, the symptoms of low metabolic energy, such as fatigue, weight issues, memory loss, cold hands and dry skin, may start to appear.
Diagnosing Metabolic Energy Problems
To restore energy to a healthy level, the causative problem(s) must be corrected. Toxic exposure, nutritional deficiencies, food allergies (such as allergies to wheat), viral factors and auto-immune damage are all, to some degree, universal. If severe enough, any one of these factors (or a combination of several lesser ones) can overwhelm the body’s metabolic mechanisms and become the cause of the problem.
The focus of this article, however, is low metabolism caused by adrenal or thyroid dysfunction, or a combination of the two.
Before going further, I wish to point out an observation I’ve made regarding the relationship of the thyroid gland to the adrenals. They seem to have an inverse relationship. How we appear (physically, emotionally and biochemically) seems to be a function of how the thyroid and adrenals relate to each other. Low adrenal function can appear like excessively high thyroid function—that is, sufferers of both may be thin and pale, nervous, have palpitations, and have unstable temperatures. By contrast, low thyroid function may have symptoms similar to high adrenal function—that is, sufferers of both may be heavier than normal, have a reddish facial complexion, have stable temperatures and a calm demeanor.
If poor thyroid function is the only cause of low metabolic function, we typically see a reddish complexion, thinning of the outer eyebrows, easy weight gain, depression, sluggishness, excessive sleep, high blood pressure and a decreased ability to fight infection. Conversely, if poor adrenal function is the only cause of low metabolic function, we typically see pallor, full eyebrows, difficulty gaining weight (if the problem is severe), difficulty losing weight (if the problem is moderate), anxiety, exaggerated startle reflex, insomnia and unrefreshing sleep, low blood pressure, allergies and autoimmune problems.
Most people have a mixture of poor thyroid and poor adrenal function rather than purely one or the other, and therefore a mixture of symptoms. Within my practice I have developed several tools that assist in diagnosing the causative problem and facilitate treatment (see sidebar, page 18). They provide very useful feedback tools for proper diagnosis and treatment of low metabolic energy.
Treatment for Low Metabolic Energy
Where do we start, with the adrenal or the thyroid insufficiency? If both the thyroid and the adrenals are weak, adrenal repair must precede thyroid repair (see the Metabolic Scorecard™, page 20, to determine whether problem is adrenal, thyroid, or both).
If the adrenals are weak, then even normal thyroid activity places an excessive burden on them. One may begin to feel “hypoadrenal” (coldness, weight loss, dryness, fatigue, insomnia, and anxiety) and then the body innately turns down its own thyroid energy production by increasing production of RT3. Conversely, if the adrenals are strong and the thyroid is weak or unable to keep up with the adrenals, one begins to feel “hypothyroid” (heat intolerance, weight gain and fluid retention, tiredness, excessive need to sleep and depression). A very common error made by medical practitioners is to focus entirely on the thyroid and ignore the adrenals. In a weakened adrenal state, prescribing thyroid medication that contains T4 and/or T3 may produce limited or transient improvement. Subsequent increases of the dose offer little or no benefit as the medication pushes the energy machinery into overdrive. Unfortunately, this higher energy level is unsustainable due to the stress on the adrenals. Eventually the adrenals become fatigued and the symptoms of low energy return.
If, however, the adrenals are functioning well, the thyroid hormones can do their job and the result is good metabolic energy. Another way of looking at this thyroid-adrenal relationship is to think of the thyroid as “generating” the energy while the adrenals need to be able to “handle” the energy. If the thyroid-generated energy is excessive for the adrenals’ ability to handle it, the body will down-regulate the thyroid energy as much as it is capable of doing to accommodate what the adrenals can safely handle. Sometimes, in an effort to help the patient feel better, the physician keeps increasing the thyroid dose or even gives a T4-T3 combination like Armour Thyroid or just a T3 support like Cytomel.
The problem with this approach is that it forces the system to function at a higher energy than the adrenals can handle. Initially the adrenals have enough reserve to handle the higher thyroid energy so the patient feels better. When the (adrenal) reserves are exhausted (this can happen within a few days, weeks or months) the patient can develop fatigue, anxiety, bursts of rapid heart beat or the feeling of such bursts (palpitations) or other symptoms of either high thyroid function or of low adrenal function (see the Metabolic Scorecard™). This is the “crash and burn” phase of a thyroid treatment that ignores the adrenals’ capacity to handle the thyroid support. It is often followed by a recommendation for an anti-anxiety or anti-depressant drug.
Adrenal Repair Basics
In general, stress hurts the adrenals. We can define stress as anything that challenges our survival, joy, prosperity, security or stability. It is anything that forces our system to adapt, such as change of circumstances, temperature extremes, changes in biochemistry (as in a sudden change of supplements, medication or even change of diet). Infection, lack of sleep or even lack of love are stressors. Mold is a common serious stress but difficult to avoid.
The opposite of stress, such as joy, adequate sleep and rest, comfort, peace, security, stability and good nutrition, are examples of factors that help the adrenals. So the obvious approach is to avoid the stressors and seek out those things that help.
As far as diet goes, it is important to eat more proteins and good fats (not vegetable oils) and to limit carbohydrates, especially sugars. Avoid stimulants and physiologically stressful substances such as caffeine, diet pills, chocolate, alcohol and cigarettes. If you have allergies, avoid the allergens; common allergens are wheat and dairy. Although this may sound surprising, we actually tend to crave foods to which we are allergic.
Metabolic activity (the chemical processes and changes going on in our body) represent a stress. At a level that can be handled by the adrenals, this stress is good for us—called eustress—and maintains life. If metabolic activity is too strong for the adrenals, for example, from excessive thyroid stimulation, then the stress is bad for us—called distress—and wears the adrenals down.
Even “good stress,” such as celebration, can sometimes be excessive for the adrenals. Look for opportunities to experience security, joy and optimism. Learn to avoid negative emotions such as anger and fear (for example, horror movies). Increase rest; get as much sleep as possible and make the timing as regular as possible. Pushing too hard, excessive work or exercise and any sleep deprivation stresses the adrenals.
Adrenal Support
Providing the body with proper support in the form of good nutrition is critical to repair. The minimal nutritional requirements for healthier adrenals are:
A healthy whole foods diet that is organic, contains an adequate amount of protein and healthy fat (oil is liquid in room temperature while fat is solid in room temperature) and adequate fat-soluble vitamins, while omitting anything you are allergic to, such as wheat, dairy or other specific foods.
B-complex vitamins: A very complete B-complex with lots of vitamin B5 (pantothenic acid) may be necessary. Remember that fermented foods are rich in B vitamins.
Vitamin C and antioxidants: Vitamin C is critical to adrenal function. The buffered powder form of vitamin C is often most easily tolerated as part of a drink sipped throughout the day. It is important to take bioflavonoids with vitamin C as these help recycle and sustain the antioxidant activity.
Amino acids: Individuals with weak adrenals often cannot digest meat or proteins into amino acids very well. The adrenals thrive on amino acids. As with the vitamin C, amino acids are best taken as part of a drink sipped throughout the day.
Healthy fats: Animal fat is the best source of healthy fat but it must be organic. If dairy or meat, the animal should, if possible, be grassfed. Eggs are also healthy. Free-range hens are the best source. Cod liver oil provides vitamin A, essential for the production of adrenal and thyroid hormones.
Unrefined sea salt: This helps the adrenals by raising low blood pressure and ensuring the body retains water. Plain table salt (sodium chloride) does not contain the same minerals and some people feel poorly when using it.
Restoring Thyroid Function
For mildly poor thyroid function, one can often get the needed support with supplements such as L-Tyrosine and iodine (for example, Prolamine Iodine from Standard Process) or a thyroid-supporting glandular supplement (for example, the product called T-100 Thyroid Glandular Support). Supplements containing mixtures of thyroid nutrients are also available. Some thyroid glandulars may offer more complete support.
If the thyroid condition is more severe, one may require prescription medication. Giving only T4 (such as Levothyroxine, Synthroid, Unithroid, and Levoxyl) is a good choice if T4 is the only missing component. In individuals with poor conversion of T4 to T3, a desiccated thyroid preparation (such as Armour Thyroid Rx) often works best because it contains the needed T3 as well. Breaking up the dose into two or three doses daily provides a more stable blood level of T3 and generally produces better results. Taking the daily dose all at once in the morning tends to be stressful on the adrenals and often leaves one feeling depleted by afternoon. Evidence of this fact can be seen when taking daily temperatures. The adrenal stress shows up as increased temperature volatility.
Note that if the adrenals are too weak to handle the desiccated thyroid, then we often see an initial response of better energy and fewer symptoms, followed by a later crash in which energy can drop to even lower levels than before the desiccated thyroid support. Additionally, other symptoms of adrenal stress such as anxiety, insomnia and palpitations (racing heart) can then occur. The same can be seen with fast release T3 (such as Cytomel) or with slow release T3.
Estrogen Dominance Support (For Women)
Estrogen is generally a stimulant and estrogen dominance presents as anxiety, agitation, muscle tension and increased cell division in female organs, leading to uterine fibroids and breast cysts. Conversely, progesterone has a calming effect, including sedation and slowed cell division. An imbalance that favors a predominance of the estrogenic effect (either excessive estrogen or insufficient progesterone) is called estrogen dominance. (See below).
Metabolic Therapy™ Healing
As you can see, low metabolic energy can appear as any of numerous symptoms. The best way to eliminate the symptoms is to correct the underlying problem—in most cases, poor thyroid and adrenal function. Once you’ve made the choice to correct the problem, some general principles of treatment apply:
If the treatment is working, one should feel improvement as time goes on. Healing crises rarely occur with thyroid and adrenal repair. They tend to occur more often with detoxification or elimination of a biological agent.
Successful treatment is achieved more easily through the use of feedback based on changing signs, symptoms, temperature patterns and lab values.
When taking supplements, especially for those who are highly sensitive or have allergies, the old nursing adage of “start low, go slow” is very important to remember when restoring adrenal and thyroid function.
It is the adrenal component that is least understood or appreciated. Yet both thyroid and adrenal function can be enhanced using good nutrition, lifestyle changes and, in some cases, supplements and thyroid medications. These can help you start living a normal, symptom-free life.
SIDEBARS
Symptoms of Low Metabolic Energy
Although many of the symptoms below seem unrelated, they may all stem from the same root problem of low metabolic energy.
GENERAL: Low body temperature. Coldness. Low energy or fatigue. Weight problems (can’t lose or gain it). Slow healing.
BRAIN: Depression and/or anxiety. Poor memory, focus or concentration. Sleep disorders.
IMMUNE SYSTEM: Under-reactive or over-reactive; that is, frequent infections (skin, sinus, bladder, bowel and yeast problems); allergies; auto-immune disease.
MUSCULOSKELETAL: Fatigue, fibromyalgia (muscle or joint pains); generalized aches and pains; repetitive use injury and carpal tunnel syndrome. Weak connective tissues (ligaments, bones, etc.); headaches.
SEXUAL: Loss of libido and function; menstrual disorders; infertility.
VASCULAR: Low blood pressure; high blood pressure; Raynaud’s disease.
BOWELS: Constipation; gas or bloating; digestive disorders; irritable bowel syndrome (IBS).
NERVOUS SYSTEM: Numbness of hands and/or feet (usually symmetrical); dulling or loss of senses such as vision, taste or smell.
SKIN: Dry; pallor in light skin, darkening or dark patches in dark skin; acne.
HAIR: Brittle, falling, coarse, dry or oily.
Useful Diagnostic Tools
METABOLIC SCORECARD™: A method for looking at symptoms to provide guidance on whether there are adrenal, thyroid, or a mixture of problems. (See below.)
METABOLIC TEMPERATURE GRAPH™: A method for measuring and interpreting daily temperatures to gain insight into metabolic energy issues associated with both adrenal and thyroid function. (See below.)
THYROID SCALE™: A method of evaluating thyroid lab data (TSH, Free T4, and Free T3) relating them to optimal values as well as to one another. This provides a clearer picture of what is going on as opposed to the old, “Your lab values are all normal” response. (See below.)
ESTROGEN DOMINANCE QUESTIONNAIRE: A method of looking at symptoms to determine whether an estrogen/progesterone imbalance might be causing metabolic problems. (See www.drrind.com/therapies/edquestionnaire.pdf.)
Common Thyroid Conditions
HASHIMOTO’S THYROIDITIS is a common autoimmune condition in which one develops an allergy to one’s own thyroid gland. In the early phase, when there is destruction of thyroid gland and spillage of thyroid hormone (T4), there is a hyperthyroid effect. In an effort to lower the T4 level in the blood, the pituitary gland decreases the amount of TSH it secretes, producing low TSH values. The hyper-metabolic state that occurs usually stresses the adrenal glands and causes adrenal fatigue. When enough destruction has occurred and the thyroid gland can make only a small amount of T4, one goes into a hypothyroid phase. Now one has hypothyroidism and adrenal fatigue. Autoimmune antibodies, namely antithyroglobulin antibodies (ATA) and thyroid peroxidase antibodies (TPO), are almost always present on blood testing. The body can eventually counter the hyper-metabolic state by reducing the conversion of T4 to T3 (and increasing T4 to RT3 conversion). Thus metabolically, this is like stepping on the brakes in a car that’s going too fast.
GRAVES’ DISEASE is an autoimmune disease in which an antibody is produced that mimics TSH. It signals the thyroid gland to make T4. As the T4 level rises, the pituitary tries to reduce the T4 level by reducing TSH levels and we get a low TSH. Typically we find elevation of thyroid stimulating immunoglobulin or TSI. Most labs consider a level of 130 or higher as evidence of Graves’ disease. In reality, we often see the signs of hyperthyroidism begin to appear in a subtle way at a level of 90. At 110 the symptoms are easier to see. By the time we get to 130, the symptoms are usually severe. Unlike Hashimoto’s thyroiditis, in Graves’ disease the T4 goes into high conversion to T3. This is like driving a car too fast and stepping on the accelerator. This condition is extremely stressful to the adrenal glands.
The Metabolic Score CardTM
Are my metabolic energy problems due to low adrenal or low thyroid function? The Metabolic Scorecard™ provides valuable insight as to whether low thyroid and/or adrenal function may be the cause of your signs and symptoms. Below is a sampling of items from the Metabolic ScorecardTM. This will tell you if your condition is predominantly low function of thyroid, adrenals, or a mixture of both. Nobody has all the symptoms; however, the more severe the problem the greater the number of symptoms will be present. For the full chart with extensive notes, go to www.drrind.com/therapies/metabolic-symptoms-matrix.
| SIGNS & SYMPTOMS | ADRENAL | MIXED | THYROID |
| Body Type | Mild: Gains weight easily Moderate: Can’t lose weight Severe: Thin, can’t gain weight |
Gains easily, goes to tummy/hips first, very hard to lose | Weight gain, generalized or global, extremely hard to lose |
| Eyebrows | Tend to be full | Normal to sparse | Very sparse outer 1/3 to 1/2 |
| Facial Coloring | Tendency to pallor, especially around the mouth. In dark skin, it darkens around mouth, forehead, sides of face | Pallor around mouth (more visible with light skin) | Ruddy or rosy complexion, including around the mouth |
| Pigment Distribution | Vitiligo (white spots or patches) in late stage. May tan too easily. In dark skin, darker on forehead, sides of face, around mouth and chin/jaw | Milder version of vitiligo and dark patches if dark skin | In pure hypothyroidism, vitiligo and hyperpigmentation are very rare |
| Light Sensitivity | ++ | + | – |
| Temperature Pattern | Poor thermoregulation (hot when it’s warm, cold when it’s cool). Tends to low body temperatures, 97.8 or lower. Fluctuating pattern | Fluctuating pattern, usually averaging 97.8 but can be lower | Stable, non-fluctuating patterns, average can be from low 90s to a little below 98.6 |
| Emotional Reactivity | Hyper-reactive (over) | Moderate | Hypo-reactive (under) |
| Intuitive | ++ | + | +/- |
| Depression | + | ++ | +++ |
| Dietary Habits | Often leans towards vegetarianism, or avoids certain foods | Fewer dietary restrictions than pure adrenal type | Tends to eat everything |
| Bowel Function | Tendency to be irritable or hyperactive, transit time may be too fast, causing poor digestion | Poor/mixed | Tendency to constipation, slow transit time and poor mechanical digestion |
| Cravings | Sweets, carbohydrates, salt, black licorice | Mixed | Fats |
| Blood Sugar | Tendency to hypoglycemia. May need many small meals or crash | Can range from mild hypoglycemia to hyperglycemia | Normal to hyperglycemia |
| Blood Type | Most are type A | Often type O |
The Metabolic Temperature GraphTM
If you suspect thyroid or adrenal insufficiency, the first step is to take your temperature. Not to determine whether you’ve got a fever; rather, temperatures reflect an individual’s metabolic energy state.
The average daytime temperature of a healthy individual is 98.6, thus making 98.6 the optimal (as opposed to normal) temperature. Lower-than-optimal temperatures reflect a lower-than-optimal metabolic state, which is usually controlled by the thyroid mechanism. Wide variability of temperature reflects an unstable or fatigued adrenal system. Thus, on the road to health, one wants to go from low and/or unstable temperatures to 98.6 and stable temperature.
The Metabolic Temperature GraphTM is an extremely valuable feedback tool that provides a roadmap with which one can see whether one is moving toward or away from a healthy metabolic state. It provides insight as to whether or not the therapeutic efforts are working. This feedback helps guide the treatment program on a daily basis. Once corrective actions are underway, the temperature pattern will show you how your health is progressing.
Temperature Patterns in Response to Adrenal Therapy
Adrenal fatigue is characterized by unstable temperatures (A in graph below). Core temperatures have wide variations. They tend to rise in warm weather and fall in cold weather.
With adrenal support, adrenal function improves and variability decreases, that is, temperatures become more stable (B). They may stabilize in the low range (C) and then rise as improvement continues (D). The goal is stable temperature in the optimal range (E), typical of a healthy metabolic state.
If the adrenal support is working well, phases A through D can each last from one week to several months, depending on the individual. In any given individual each of the phases seems to last approximately the same length of time, some going through each period quickly, and others taking more time to go through each phase. Some phases can blend together. For example, A and D can combine into an upwardly stabilizing pattern without C being present. I have actually seen some people go directly from A to E. To go from A to E can take as little as one to two weeks or as long as a few months. The goal is for phase E to be permanent. If the adrenal fatigue is more severe (usually of longer duration), each of phases A through D tends to last longer and phase E tends to be less secure. If no progress is seen within several months, there is usually another problem present, such as toxicity or nutrient deficiencies.

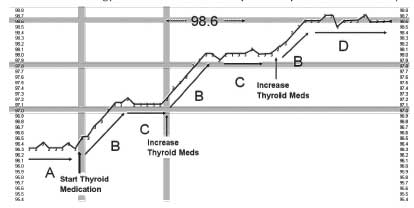
Temperature Patterns in Response to Thyroid Therapy
Below is a typical temperature pattern found in a person receiving proper thyroid support, having an average to good response. When there are only problems with the thyroid gland, the straight-line pattern is amazingly consistent.
The typical patient with poor thyroid functions has a stable but low temperature that reflects lower than optimal thyroid activity (A in graph below). After starting or increasing the dose of thyroid hormone replacement medication, the temperature steadily rises (B). The temperatures plateau at the metabolic level reflecting the current dosage of thyroid replacement medication (C). Eventually when the proper dose of thyroid replacement medication is reached, the temperature is stable at 98.6 (D). If the adrenals cannot handle this level of energy, we tend to see an expansion pattern followed by a drop in temperature.
The Metabolic Temperature GraphTM is a powerful tool that graphically depicts our metabolic state (adrenal and thyroid) and guides us on the path to recovery. It lets us know if a therapy is helping or hurting us and by how much. As your adrenals and thyroid receive the needed support, monitoring your own progress with this tool will multiply the benefits. For details on how to take your temperature and record them in graph form, visit www.drrind.com/therapies/metabolic-temperature-graph.
Thyroid Basics
The thyroid gland is located at the base of the neck and makes thyroxin (thyroid hormone or T4) which signals the cells to make energy.
The adrenal glands are located on top of the kidneys, they make many hormones (cortisol, DHEA etc.). Their main function is to help us deal with stress or help us survive. They help maintain stability of many bodily functions (physical, emotional, thermal, hormonal etc.). When there is stress—anything physical, chemical, emotional, nutritional or lifestyle such as sleep patterns, which causes us to have to adapt—the adrenals need to work. Excessive stress can exhaust them. One often overlooked adrenal stressor is thyroid energy in excess of what the adrenals can handle.
The pituitary gland is situated at the base of the brain (above the roof of the mouth). It sends out instructions to many glands, including the thyroid gland, telling them how much hormone to produce. One such hormone is TSH (Thyroid Stimulating Hormone) which signals to the thyroid gland to make thyroid hormone. The pituitary gland determines how much TSH to secrete (that is, how much thyroid hormone to tell the thyroid gland to make) based on (1) how much thyroid hormone is available; (2) how much thyroid hormone the body needs; and (3) how much thyroid hormone the body (actually the adrenals) can tolerate.
Thus a high TSH level is the pituitary gland’s way of saying that it has a high need for thyroid hormone or that the body can tolerate more thyroid energy than it is getting, and it is meant to generate more thyroid hormone production. Conversely, a low TSH reflects either a low need or desire for thyroid hormone or a low tolerance for the thyroid hormone, and it is meant to reduce thyroid hormone production. An optimal value of TSH means the thyroid hormone levels match the body’s energy needs and/or ability to utilize the energy.
The thyroid gland makes a hormone called T4 (thyroxine). T4 will become T3 (triiodothyronine) which causes energy (in the form of ATP) to be made in each living cell. T4 can also become reverse T3 (RT3) which interferes with the energy production in the cell. Just as a car needs an accelerator and brakes for proper function, the same is true for the body. The body needs T3 (the accelerator) and RT3 (the brake) to manage its energy needs.
To summarize, T4 has four iodine atoms and it is a pro-hormone, that is, it lives to become either T3 or RT3. When the body needs energy, it removes an iodine atom from the T4 and turns it into T3, which in turn signals living cells to make energy (ATP). T3 allows the body to turn up the energy when it needs to. Reverse T3 (RT3) is made by the body to tone down energy. It is made by removing a different iodine from T4. Like placing a bad key in the ignition, it blocks the T3 (the working key) from signaling the cell to make energy. It allows the body to turn down the energy when it needs to. Rather than looking at the values as low-normal-high, we can make more sense of the data if we look at each value as it relates to the optimal value. In my practice, I have found the following to correspond to the healthiest segment of the population and which I do not fine to be associated with symptoms of thyroid excess or deficiency. First, a word on thyroid tests.
Thyroid hormones (T4, T3, and RT3), once released into the bloodstream, exist either as protein-bound or in a free form. Protein acts as a sponge or reservoir to which hormones bind and then can be freed. Hormone in free form is available to interact with a cell’s receptor site to produce its hormonal effect. It is only the free form hormone that is biologically available or active. When the hormone is bound to a protein it is restrained from interacting with a cell’s receptor site.
I typically test for the following: free T3, free T4 and TSH. If there is a suspicion of Hashimoto’s thyroiditis, I include a thyroid peroxidase antibody test (TPO) and an antithyroid antibody test (ATA). I also use this to monitor the severity of the Hashimoto’s thyroiditis and to see whether therapy is working. If there is suspicion of Graves’ disease, I include TSI. Based on my observation of nearly 5,000 patients and the lab test values that my healthiest patients tended to have, I believe the optimal values for these tests, within a 5-10 percent margin of error, are as follows:
| Test | Lab Low | Optimal Range | Lab High |
| TSH | 0.5 | 1.3-1.8 | 5.0 |
| Free T4 | 0.8 | 1.2-1.3 | 1.8 |
| Free T3* | 230 (2.3) | 320-330 (3.2-3.3) | 420 (4.2) |
*Some labs divide FT3 results by 100 thus 230 is the same as 2.3, etc.
In the cases of Free T4 (FT4) and Free T3 (FT3), the optimal zone is roughly half way between the usual lab normal low-high values. In the case of TSH, the optimal zone is skewed far toward the low end of the standard lab Low-High range. For further details, visit www.drrind.com/therapies/thyroid-scale.
Thyroid Scale Interpretation Matrix
The Thyroid Scale Interpretation Matrix can be an extremely useful tool, especially when combined with the Metabolic ScorecardTM and the Metabolic Temperature GraphTM (pages 20-21). For more details, visit www.drrind.com/therapies/thyroid-scale-matrix.
| STATE OF HEALTH | TSH | T4 | T3 | TEMPERATURE PATTERN | COMMENTARY |
| Healthy | Optimal | Optimal | Optimal | 98.6, stable | – |
| Adrenal Fatigue | Low | Low | Low | Low, average is typically 97.8 or lower. | Symptoms: Predominate in adrenal column. Often confused with hypothyroidism because of low T4 and T3. Some doctors mistakenly interpret the low TSH here to mean pituitary trouble |
| Estrogen Dominance (ED) | Low | Low | Low | Very unstable | Is the same as adrenal fatigue in that they are related to each other. In adrenal fatigue, the adrenals often sequester the progesterone to help make cortisol. The drop in progesterone creates the progesterone-estrogen imbalance called ED. |
| Hypothyroidism due to low thyroid function as a primary cause (such as surgical removal of thyroid with insufficient replacement of T4) | High | Low | Low but to the right of T4 | Low, average is typically 97.8 or lower and unstable | Note there is high conversion of T4 to T3. There is a high demand for T4/T3 (high TSH) and the body is extracting as much T3 out of the T4 as it can. |
| Hypothyroidism due to low pituitary function | Low | Low | Low but to the right of T4 | Low and very stable | Looks just like primary hypothyroidism but TSH is low. We know there is demand because of high conversion of T4 to T3 but the TSH doesn’t rise to help T4 production. |
| Late Hashimoto’s thyroiditis or hypothryoid and adrenal fatigue | Optimal to high | Low | Low and mildly to the right of T4 | Low and very stable | The most common presentation of disease. Similar to adrenal fatigue but symptoms are predominantly in the mixed column. |
| Early Hashimoto’s thyroiditis | Very low | High | High but to the left of T4 | Low and unstable | The body can slow down metabolism (step on the brakes) by shifting conversion of T4 toward RT3 and away from T3. Thus we see T3 is to the left of T4. |
| Graves’ disease | Very low | Very high | Very high and to the right of T4 | Can range from below 98.6 to slightly above | T3 to the right of T4 (that is, high conversion of T4 to T3) is like a car that’s speeding out of control and the driver steps on the accelerator. This is typical for Graves’ disease. |
| Poorly effective thyroid hormone | Mildly high | High | Optimal and to the right of T4 | Tends to be above 98.6 and stable in the early phase. Later, drops below 98.6 and becomes unstable. | Can be due to nutrient deficiency, viral damage to mitochondria, toxic burden, or poor receptor site (to thyroid hormone) sensitivity. |
| Chronic infection | Optimal to mildly high | Optimal to mildly high | Optimal to mildly high | Low and moderately stable | Source of infection may be elsewhere. |
| On thyroid support that contains T3:-Desiccated thyroid such as Armour thyroid,-T4/T3 mixtures such as Thyrolar,-Slow release T3 (compounded),
-Pure fast release T3, such as Cytomel |
Optimal if dose is proper. High if dose is too low. Low if dose is too high. | If the TSH is optimal, the T4 will be low. | If the TSH is optimal, the T3 is high. | Mildly above 98.6 | The body seems to do better with a steady state of energy. T4 acts slowly but T3 is rapid to come and leave. Therefore, to maintain a steadier blood level of T3, it is best taken in divided doses. Splitting the daily dose into 2 or 3 portions stresses the adrenals less than taking the entire dose once daily and therefore leads to more stable temperatures. |
The Estrogen Dominance-Adrenal Fatigue Connection
Adrenal fatigue and estrogen dominance (ED) are very similar in their symptom presentation and share a lot in common. Most women who have one tend to have the other to some degree. Estrogen dominance and adrenal fatigue have the following relationship:
Progesterone is transformed into cortisol as well as into other hormones.
Most ED is due to insufficient progesterone and therefore accompanies low cortisol production.
Most adrenal fatigue involves an inability to keep up with cortisol production.
When adrenals are stressed, the increased need for cortisol depletes the progesterone levels in making cortisol. As more progesterone is shunted or sequestered to make cortisol, less is available to balance the estrogen. Another common reason for low progesterone levels is an anovulatory cycle (a menstrual cycle in which there is no ovulation). Without the ovulation there is no corpus luteum to make additional progesterone for the cycle. The lowered progesterone level leaves us with an excessive estrogenic effect due to deficiency of progesterone.
In summary, fixing adrenal function and estrogen dominance go hand-in-hand and it is therefore difficult to fix one while ignoring the other. ED can also be caused by excessive estrogenic stimulation. Typical sources of estrogenic effect are:
Excessive fatty tissue: Fat cells make estrogen and estrogen causes fatty tissue growth. This is a vicious cycle we’d like to avoid.
Hormone replacement with non-bio-identical hormones such as estrogens from horses or chemically modified estrogens. These have very potent estrogenic effects. This is especially problematic if there is no (calming) progesterone given at the same time to balance the (excitatory) estrogen. Unopposed estrogen is a powerful cause of ED. Synthetic or non-bio-identical estrogens would more appropriately be called estrogenoids (substances that have an effect similar to estrogen) as they are not truly the estrogen our body makes. Progestins are often given along with synthetic estrogens. These are chemical substances whose effects are similar to progesterone but act differently from progesterone because they are chemically different. Our bodies cannot convert the progestins into cortisol to help the adrenals or convert them into any other hormonal compounds as we could with bio-identical progesterone.
Exposure to chemicals that mimic estrogen such as many plastics (e.g. microwaving food in plastic dishes or using plastic wraps and containers) or from eating soy products or non-organic food. Feedlot livestock are typically given potent estrogenic substances (“super-estrogens”) to make them more productive. Our produce is often laced with these substances and soy foods are very high in estrogen-like compounds.
Correcting ED involves more than just correcting the estrogen-progesterone balance and supporting the adrenals. It is important to eliminate the causative factors as much as possible. Excessive exercise, insufficient sleep, toxic exposure, poor nutrition (high intake of carbohydrates, low intake of fat and protein, low intake of nutrients), and stress are some common causes.
Direct help to the adrenals indirectly helps improve the ED (estrogen-progesterone balance) by allowing more progesterone to be available to offset the estrogen. Direct help to the estrogen-progesterone balance indirectly supports the adrenals by making more progesterone available for cortisol production. In addition, progesterone itself has a toning- down, calming and sleep-supporting effect which further helps stressed adrenals.
If we want a very gentle support for progesterone production we can try the herb chaste tree (1-2 tablets early each morning upon waking). This is typically helpful for menstruating women with estrogen dominance. Herbalists often use this to help produce more regular ovulation and subsequently improve progesterone production. The herb is often helpful in relieving menopausal symptoms (hot flashes) when taken in combination with black cohosh.
I find that the easiest way to restore balance to estrogen dominance is with progesterone. I’ve developed a progesterone protocol for doing this which helps most of my patients. There are always some who might respond poorly for which corrections need to be made. That is why it is always advisable to work with a physician who is familiar with the use of natural hormones while trying to restore a physiological hormonal balance.
It is important to note that there are different ways to take progesterone and these affect patients differently. Dosage is also an important factor. As with any hormone, optimal dosage is the key. Too much or too little will either not produce the desired result or actually produce an undesirable result. This is an important consideration when post menopausal women use progesterone for the first time. The progesterone will temporarily increase the body’s sensitivity to estrogen (estrogen receptors temporarily become more sensitive to estrogen) thus producing a temporary increase in estrogenic effects. This can produce a temporary worsening of symptoms. To minimize this effect, progesterone needs to be started at a very small dose that is increased slowly to full dose over 2-4 weeks.
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly magazine of the Weston A. Price Foundation, Summer 2009.
🖨️ Print post
Black mold complications
Is household black mold a contributing factor to adrenal problems? I have been asked by my readers what implications exposure to black mold in their homes might have. Thanks.
black mold
What information do you have about black mold and adrenal problems?
Thanks
Hypothyrodism in infant
Hello,
My niece was diagnosed with hypothyroidism at birth. She is on a synthetic drug, and they say she will be on it for the rest of her life. What advice do you have for her?
Gina
Where to find a doctor who thinks outside the box and understands all this. Listens to your history, knows what tests to order and how to properly treat them. Tuolumne County, CA
look for functional medicine/integrative medicine practitioners. You can actually look on the IFM https://www.functionalmedicine.org/practitioner_search.aspx?id=117
Another resources is A4m http://www.a4m.com/directory.html
Most of the providers with this type of training will require cash visits. Insurance doesnt pay for us to sit and talk to you and find the root cause of the disease, order proper tests etc.
hope that helps.
Where can I find a doctor in my area 25414?
I have been letting go of my problem. I found out in 2004 by Dr. Finlayson that I had a Thyroid problem. Armour was the solution at that time and was the same for some years later until the Armour I had changed and I had to find another solution. I have had many problems all these year and had different prescriptions that did not work,and horrible doctors that I had to stay away from and ended up with a Meningioma Brain Tumor on the left side of my head removed 7/3/07.
Lost weight when I came home there was deep problems with the Drugs they tried to give me in Lexington Rehad Center and I was able to stop it and go to a Devonshire Retirement Building for 10 days and go home. I was dow to 106 lbs LOST 20 LBS.
I have a problem with trying to keep in my mind that I have a THYROID PROBLEM. I have had 6 Doctors that told me about it…But My Body has an Off and On Session that makes me think that It Isn’t my THYROID….
I do not have all those Symtoms…..But I do get the Pituitary Low Blood Test, But Doctors DO NOT EVER GO INTO THAT AREA, ONLY GO INTO HYPOTHYROID.
I have been taking American Biologics Thyroid Glandular, But off and on….Why it takes 8 tablets and now capules to actually work for my BODY and MIND…..
NO TO AMOUR It did not do the job for me…..I found American Biologics Pituitary Glandular and have started to take that but find that THERE IS another Problem….
DO you know what causes the Pituitary to not be balanced, so the Thyroid will Stay healthy..
I have Had a low THyroid Way Before 2004 but never saw a DOCTOR that could tell me the Problem.
I have 3 other Problem way before that were related to Thyroid I never knew what I know now.
CAN YOU GIVE ME ANY OTHER SUGESTIONS?
I suggest joining one of the groups associated with Stop The Thyroid Madness.
Are you having a yearly MRI to make sure that your tumor does not grow back? Are the doctors checking your pituitary at that time too? There is a pituitary clinic at Strong Memorial Hospital, Rochester, NY. They need a referral from your doc, along with certain blood tests to be done and an MRI with/without contrast. When in doubt, check it out. Susan
Hi there, I thought that I have the same issue , but I refuse to take medications for my thyroid. My tsh was slightly elevated 4,49 and I had anti thyroid antibodies who were attacking my thyroid.
I found out recently that gluten has the same properties as the thyroid cells and the body doesn’t know what to attack., and it attaks the thyroid also whan you consume gluten. I’m more than 4 months off the gluten and my tsh dropped to 2 now..
I wold like to see this article from dr rind..and anything else he has maybe a book.. very informaitve thank you.
My son has thyroid problems and has his thyroid monitored regularly. Although the doctor tells him his levels are within range he continues to have severe pain in his throat, joint pain and IBS. He had the top half of his left kidney removed due to cancer. Can adrenal complications be contributing to his symptoms?
From above comment by Elizabeth:
I found out recently that gluten has the same properties as the thyroid cells and the body doesn’t know what to attack., and it attaks the thyroid also whan you consume gluten.
I’m 31, female. I’ve been diagnosed with adrenal fatigue, estrogen dominance + low progesterone and high testosterone, a slew of gastrointestinal disturbances, and low vitamin D (31ng/mL). What key ingredients do you recommend to look for in an adrenal supplement? (Or can you recommend any brands outright?) I was on high doses of a B complex that also contained rhodiola and lamb pituitary for 8 mos, but I saw no improvement (got worse like I do every winter). That supp was $54/bottle, so I recently switched to a B50 supplement. For my hormones, I use vitex, DIM + CDG, and progesterone cream. I also use several other standard supplements not targeted at adrenals or female hormones- too many to list.
Also, could adrenal fatigue be the reason I wake up every night after 3-4 hours?
I fall asleep easily, but when I have a nocturnal awakening, I cannot get back to sleep. My heart is usually racing, and I’m too alert. GABA helps my heartrate calm down, but I still can’t fall back asleep. Then I’m tired all day until evening, when I get wired. I’m in a constant fight/flight, and too tired to work out anymore. (I try to do gentle yoga though). Could the nocturnal awakening could be adrenal or cortisol related?
I have had similar problems with insomnia, and I have PCOS so I can relate. I have felt much better going low on the carbohydrates, high on organic animal fats (butter, tallow, lard, and egg yolks, at least 96 g fat per day FAT is your FRIEND when it comes to cortisol and sex hormone balance!!), moderate/high organic protein (beef, chicken, bacon) and also taking Her Package (beef ovaries, kidney, uterus and Fallopian tubes) from Heart & Soil along with a 500 mg dose of ashwaghanda in the evening to help me become tired at night enough to fall and stay asleep. I never wake up in the night anymore.
Her Package and this diet improved, for me, labour pain equivalent periods and PMS. For severe constipation & IBS symptoms, and gallbladder/stomach acid issues, I take the Thorne Digestive supplement that contains ox bile, digestive enzymes and betaine hydrochloride with meals, a potent trace mineral complex from seawater (for magnesium to help bowel movements and boron for hormone production primarily), Lugol’s 5% iodine (for thyroid support) and ginger for a gentle laxative for now while I figure things out. Organic matcha green tea and taking slow, 1 hour walks in the fresh air also helps to lower cortisol.
This article has given me the answers that I’ve been looking for and more! I’m grateful to have come across it.
I have read your article over and over. Your description of the thyroid medications and the adrenal crash was like I had wrote the article. I crashed so bad, my husband and I were sure that I was having a heart attack and so did the ER. Here where I live, I am having a hard time finding a doctor or specialist that will listen and not depend on blood work as the gospel. I go from doctor to doctor trying to get someone smart enough to put the puzzle together. I don’t think they are out there. Sad. . so sad!!