






A Modern Detective Story
As presented at Wise Traditions Conference 2012
We know of eight trace elements that are essential to human health. Iodine, as we all well know, is essential for thyroid function; iron is essential for hemoglobin synthesis; and copper is essential for collagen synthesis. Chromium is involved in glucose metabolism, although it is not very well established how important it is for management of diabetes. Selenium is very important because it is a part of glutathione peroxidase, which works as an antioxidant. Fluoride is not essential for life but considered important for dental health. Manganese is also considered to be essential as it is involved in cartilage synthesis; however, it’s deficiency has not been observed.
As for zinc, its recognition as an essential mineral came only recently. The story of how zinc achieved acceptance is a very interesting one. Not long ago scientists derided the premise that zinc played a role in human health. Today we know that zinc plays many important roles. For example, zinc is a part of the super oxide dismutase enzyme, so it also has a role as an antioxidant. In addition, zinc takes part in neurotransmitters, and plays a key role in immune function, sound growth and development. In fact, zinc is really a miracle element in many ways.
EARLY ZINC RESEARCH
The first hint that zinc played an important role in life processes came in 1869, when the mineral was found to be essential for the growth of a fungus, Aspergillus niger. It was a chemist from the University of Lyon, France, Professor Jules Raulin, who reported in 1869 that zinc was needed for the growth of this organism. Prior to that zinc was not considered to be important for biology.
In 1926 scientists found zinc to be essential for the growth of higher plant life, and in 1934 Wilbert Todd, Conrad Elvehjem and Edwin Hart from Wisconsin reported that zinc was also important for growth in rats. In 1955, a disease called parakeratosis in swine was reported by Tucker and Salmon, who showed that zinc could cure skin lesions. And then O’Dell and Savage showed that zinc was needed for the growth of poultry in 1958.
HOW I CAME TO STUDY ZINC
I was born in India, and some years later I came to the University of Minnesota (USA) for my medical training. In 1958, I finished my training, received my PhD and became a hematologist. At that time, I was contacted by Professor Hobart Reimann, Chief of Medicine at Jefferson at that time and formerly Chief of Medicine at Minnesota. He was invited by the Shah of Iran, who was a personal friend, to set up a medical curriculum for a university in Shiraz, Iran. And he was looking for some young person who could go and help him set up the curriculum.
Cecil Watson, who was my boss, said that perhaps I might be interested in doing this job. Hobart contacted me, but I was reluctant because my research was going very well at the University of Minnesota, I was happy, I did not speak the Iranian language, and I had no interest in going to Iran. So I said to Hobart, “Hobart, why do you want to disrupt my career for two years for something that would be a waste of my time?”
But he was a very convincing person. He told me, “You’re a young man, you should go for two years. You never know what you will see in terms of diseases, and you’re a clinical investigator. You might enjoy seeing something new. If nothing else happens, you will at least see a different country.”
I finally accepted his challenge, went there and within two weeks of my arrival, an Iranian physician presented a patient to me in a medical center grand rounds. He was twenty-one years of age but looked like an eight- or ten-year-old boy. He had extremely retarded growth, he had hypogonadism, that is, no secondary sexual characteristics (his genitalia were infantile) and the skin on his face appeared rough.
Superficially, it looked as if he might have suffered from vitamin A deficiency, but we ruled this out later. He also had anemia; his hemoglobin was 5 gram percent. As a hematologist, my first job was to look at the red blood cells to see what was causing the anemia. I determined very quickly that the anemia was due to iron deficiency.
But there were two problems: by reading the Textbook of Medicine and Hematology I learned that adult males don’t become anemic to this extent unless there is a blood loss. And this patient had absolutely no evidence of blood loss, so my first question was; how did he become iron deficient?
And the second major problem was that I could not explain this extreme degree of growth retardation and hypogonadism based upon iron deficiency. If you take rats, pigs or even elephants and make them iron deficient, nothing happens to their growth or gonads. So those were the two puzzles that I could not easily resolve.
I also wondered how often these cases came to the attention of physicians. I was told by the Iranian physician who brought me the patient that such cases were very frequent in the villages around Shiraz; he said that if I wanted any number of cases like this they could bring them to my service.
I was located in Nemaze Hospital, a very modern hospital in Shiraz, Iran; it was actually a show piece for the Shah of Iran. I controlled twelve beds under my care, so I told them to bring me twelve patients.
And sure enough, within two weeks, I had twelve such patients. I studied them in great detail. One very interesting thing was their nutritional history. It turned out that they were eating only bread, made of unleavened flour. There was no animal protein intake; they had some vegetables but very little dairy products or animal protein.
And most interestingly, they were also eating a pound of clay every day. Shiraz is surrounded by hills and they would go there and get the clay and eat it. I’d never seen a clay-eater in all my life, not in Minnesota or anywhere else, and I did not quite understand why they were eating clay, but that was the story.
PUBLISHED PAPER
I studied these twelve patients in great detail. I did not have very good laboratory facilities in Iran but I did a very good clinical study. I put all the clinical findings in a paper entitled, “Syndrome of Iron Deficiency, Anemia, Hepatosplenomegaly, Hypogonadism, Dwarfism, and Geophagia.” I submitted this paper to Professor Gutman, the editor of the American Journal of Medicine, and it was published in Volume 31, 1961.
In that paper, I speculated that perhaps because of the high phosphate content in the clay and cereal protein, iron was being chelated. I also went to the periodic table, looked at the transitional elements and speculated that perhaps if iron is being chelated, other trace minerals may be be affected similarly. I suggested that zinc may be another mineral that is similarly chelated and thus unavailable for absorption.
Zinc was very attractive to me because of earlier studies showing that it was a growth factor for microorganisms, for plants and for animals. So I thought that if there were a zinc deficiency in humans, I was looking at it right there in Iran.
I included this speculation in the American Journal of Medicine article, and I also told the editor that if he thought that I was speculating too far or too much and he did not like it, I’d revise my article. Still, I urged him to publish the description of the syndrome because this syndrome did not exist in any textbook of medicine.
Well, Dr. Gutman was a very brave editor. He reviewed the paper himself. He wrote to me that the part he liked the most was the speculation about zinc and he did not want to remove anything I had written. The whole article was published completely unaltered. It’s a sixteenpage article with great detail and information, and includes my speculation about zinc. In 1983, this article was cited as a nutrition classic and republished in Nutritional Review. By then, zinc deficiency was an accepted phenomenon.
DWARFISM IN EGYPT
My paper attracted the attention of a lot of physicians, nutritionists and biochemists in the United States. One of them was Professor William Jefferson Darby, Chief of Biochemistry at Vanderbilt University. He liked my idea that zinc deficiency might be contributing to the symptoms and invited me to meet with him in Cairo, Egypt.
In Cairo, there is an institution called the United States Naval Medical Research Unit, which was established by Franklin D. Roosevelt for studying infectious diseases. Just before I arrived there, a Rockefeller group had worked on typhus fever. The American army used to be stationed in Egypt, and many soldiers died because of infections.
At that time, the Rockefeller group had left so the institute was available to study zinc. I went there and talked to Bill Darby, but my main concern was whether I would find these dwarfs in Egypt? I saw them in Iran but maybe this happens only in Iran and not in Egypt or any other country.
So I went with Bill Darby on a tour of several villages. I did not speak the language, but I had a translator with me. To my great surprise, I found that after visiting five villages that day, I saw three or four patients in every village who looked like eight- or ten-year-olds, but their chronological age was eighteen to twenty. It shocked Bill Darby completely. He asked me, “Why do you ask the ages?” But that was how I made my discovery.
At that point I decided to join Vanderbilt University to do the research on zinc in Egypt. I was helped by the National Institutes of Health, which gave me very good support, and also Admiral Galloway of the U.S. Navy was able to provide support for my research. In addition, I had help from the Egyptian Ministry of Public Health. With all that help I was able to set up a good laboratory where I could measure zinc.
I did not see females when I was in Iran and Egypt; the reason was that females would not come to me to be examined. They refused to come to my ward but later on I had an Iranian physician working with me who was able to examine these female dwarfs. He kept them in his own house and found that indeed they had ovarian hypo-function and were growth retarded. These results were reported in 1974 in the American Journal of Clinical Nutrition.
Zinc deficiency not only affects males but also females. Other symptoms include rough skin, poor appetite, mental lethargy, and frequent infections. Now, this last symptom is very important: I never saw a dwarf beyond the age of twenty-five in the Middle East, either in Iran or Egypt. I went to the villages, asked the physicians what happened to them, and was told that they died of infections: pneumonia, meningitis, viral, parasitic, all kinds of infections. That convinced me that zinc probably has a very important effect on immune cells.
TREATING ZINC DEFICIENCY
Back in those days, in 1961-1962, the measurement of zinc was very difficult. We did not have the atomic absorption spectrometer, so you had to do the dithizone technique. That meant shaking the tubes all day for eight hours and at the end of eight hours, you’d get two results, two patients. It was very arduous and difficult, and the contamination problem was very difficult to deal with, but in spite of these problems we were able to study forty dwarfs in great detail. Not only did we measure zinc in the plasma, we also looked at zinc levels in the red cells, hair and urine. By use of Zn-65, we also measured the zinc turnover rate and exchangeable pool.
We put all these things together and showed for the first time that indeed zinc deficiency occurs in humans. Prior to this, all the textbooks said that zinc deficiency was never seen in human subjects.
We wanted to see whether by giving zinc we could make these dwarfs grow, although I had never seen any such example in the textbooks of medicine, any instance of someone aged eighteen or twenty years who would grow just because you are giving a simple inorganic element like zinc. I did not believe it was possible; nonetheless what we gave them 15 mg of zinc a day. We studied about forty dwarfs in Egypt.
At that time zinc capsules were not available in the market. I had to take zinc sulfate and put it into a capsule. I also needed special permission from the U.S. Navy and the Egyptian government to give the dwarfs zinc. I had to argue with them that the amount of zinc I was giving was not toxic.
To my great surprise I found that within three weeks they were developing secondary sexual characteristics, they started growing hair―mustache, beard and axillary hair―and within six months the genitalia became completely normal. Even more surprising, within one year the gain in height was five to six inches.
When I saw those results, I was truly thrilled. I knew that this was something very important for medicine. We published several papers from Egypt. One thing we were able to do was to discriminate between the effect of iron and the effect of zinc. When we gave them iron, just iron sulfate, we corrected the anemia, the hemoglobin became normal, iron became normal, iron binding capacity returned to normal, but nothing happened to their growth or gonads. But when we gave them zinc they remained anemic, hemoglobin did not change, but they grew in height and developed normal adult genitalia within six months.
CONTROVERSY AND ACCEPTANCE
Those were the basic reports that we published from Egypt. Some of my colleagues praised the observation; they thought that it was a great discovery. But there were several scientists who thought that it could not happen, that zinc had no effect, and the topic became very controversial. I had to live with controversy for almost ten years. I constantly had to defend the thesis: why did I think it was zinc? As a matter of fact, some of my colleagues told me that I had become a lunatic to think that zinc was needed by humans.
In 1973, I got a call from National Academy of Sciences to appear before the National Research Council to talk about zinc. I told the chairman, “You read English, I have written everything in English, you can decide on your own whether my evidence is good enough or not.”
“We have done that,” he said, “and we all in the committee agree that zinc is important and is essential for humans, and we are planning to submit this to the U.S. Congress to declare zinc as an essential element. We need to establish the recommended dietary allowance (RDA) and we want you to tell us what the recommendation should be.” And that was a great relief for me, the controversy was ended and I had a peaceful life after that. Based on our input the RDA was set at 15 mg per day for adult males.
ZINC IN PARENTERAL SOLUTIONS
After my stay in Egypt, I came to the U.S. and started doing my work on zinc in the laboratory. At that time, there was a lot of research going on in developing parenteral solutions to give to patients who could not eat or who had malabsorption and could not sustain life. At that time, the rehydration solution and the parenteral nutrition solution (TPN) were almost as perfect as you could get for all the animo acids, vitamins, and so on. But if patients received this TPN for three months, they would die of infection.
I was shown one patient at Harper Hospital whose hemoglobin had dropped from twelve to nine. When I saw this patient, she was psychotic; she had a lot of parakeratotic lesions around her eyes, mouth and orifices, the same lesions as you see in severe zinc deficiency, in patients with acrodermatitis enteropathica. I told the resident not to worry about the hemoglobin but to worry about her life, and to give her zinc. He said, “Dr. Prasad, where do I find zinc to give parenterally?” There was no solution available so I got on the phone, called the FDA and asked their special permission to prepare parenteral zinc solution to give to this lady or else she would be dead within three to four days. They gave me permission to do that. My pharmacy helped me get the solution and the patient recovered completely.
This kind of experience had been observed by many other scientists throughout this country and also elsewhere. FDA, USDA, NIH and U.S. Pharmacopeia, they all decided to have a very urgent meeting in 1977 in Chicago, and at that time it was made mandatory for the physicians to include zinc in their parenteral solution, and this has continued to the present time. The addition of zinc has made TPN completely successful. Now you see patients who have been on TPN for five to ten years and are doing very well. This is a very important story in terms of the impact of zinc on health.
PREVALENCE OF DEFICIENCY
When I came back to the U.S., all my colleagues told me that I had described a very important disease, made some very interesting observations, but predicted I would never see zinc deficiency in the United States. “What are you going to do here?” they asked.
As a matter of fact, Professor William Bean, Chief of Medicine at Iowa University, wrote a book called Rare Diseases, and he included my syndrome in that book. I saw him in one of the meetings and I told him I liked his book very much but I thought he was wrong regarding zinc. I told him I believed that zinc deficiency was not a rare syndrome and that as time went on, we would find that zinc deficiency was more prevalent than we realized. In developing countries, zinc deficiency may affect as many as 50-70 percent of the population. The WHO estimate is that two billion people have zinc deficiency.
What about the United States? We have found that in the elderly population, 30 percent have zinc deficiency. For this reason they have immune dysfunction, they are oxidatively stressed, and they also generate increased amounts of inflammatory cytokines.
What about women during pregnancy, and the need for zinc for fetal growth? The requirement under those conditions, according to the RDA, is something like 25 mg; however, if we just look at the diet and examine how much zinc you get in a standard American diet, there’s no way that you can get 25 mg of available zinc. So there is a lot of zinc deficiency in that age group.
My colleague Harold Sandstead and I published a paper on the Mexican population of Galveston, Texas. We found that zinc deficiency affected Hispanic children and young women at rates of approximately 25-30 percent. And then Dr. Hambidge published a paper about a Hispanic group in Denver, Colorado, also showing widespread zinc deficiency. And I have seen a lot of Black Americans in Michigan, particularly the patients with sickle cell disease and others, where zinc deficiency is fairly common.
So to say that there is no zinc deficiency in the U.S. is wrong. There is plenty, but in most cases it is not recognized; you would have to be very alert to find it.
As Chief of Hematology making rounds in five different hospitals, I found that zinc deficiency was common in many other diseases. For instance, we found that patients with liver disease have hyperzincuria; alcoholics excrete a lot of zinc in their urine so they become zinc deficient; patients with malabsorption syndrome become zinc deficient very rapidly; patients with chronic renal disease also have hyperzincuria; and we find zinc deficiency in patients with nephrotic syndrome, glomerulonephritis and so on, even in several patients with malignancies.
An important question to ask is why the elderly become zinc deficient. When we started taking their history, it turns out that they rarely eat three meals a day. They have a quick breakfast, maybe a doughnut and coffee, no lunch and then they will have a meal they don’t cook themselves, often eat at a restaurant. And the intake as we calculated, in Michigan, would be around 8-10 mg of zinc per day.
Now this is not only my experience in Michigan but the same thing has been reported in the elderly from Australia, Europe and many other countries. The ainc intake is not optimal among the elderly subjects, that’s the major problem. Also it turns out that the absorption of zinc is also not optimal in this age group.
MORE RESEARCH
My next project was to set up a human experimental model of mild zinc deficiency where there was nothing abnormal except zinc intake. I succeeded in producing that model in Michigan, and we studied that model for many years, publishing many significant papers on the functions of zinc in humans.
What I did was to restrict zinc in the daily diet to around 3-5 mg. If you consider the elderly eating some 8-10 mg, it was a marginal deficiency that we were after, and that’s what we developed in the volunteers. But in spite of the fact that the deficiency was very marginal, they had a lot of evidences related to zinc defciency. For instance, neurosensory changes: they had abnormal taste, called dysgeusia. They could not taste sugar, salt and bitter properly. They had problem with dark adaptation; they had decreased serum testosterone; they developed low sperm count; and most interestingly we found that the ammonia levels went down.
It turns out that zinc is involved and zinc-dependent enzymes are required to utilize ammonia. We later proved this in our animal studies.
The subjects in our experiments had a lot of immunological changes. We found that they had decreased production of interleukin-2, a very important cytokine generated by T- helper cells. T-helper cells are a type of white blood cell that play an important role in the immune system.
The patients had decreased thymulin activity. Thymulin is a hormone produced by the thymus gland that is very important for the proliferation, development and differentiation of T-helper cells.
The thymulin story is very interesting. This hormone was isolated and found to be a nano peptide that is zinc dependent. This work was done by Jean-Francois Bach and Mireille Dardenne in France, and I went to visit them. The discovery was reported, and I wanted to see whether or not it is true in the deficiency model that I had set up.
In collaboration with Bach and Dardenne, we did a study on thymulin in our patients here. It turns out that thymulin activity is highly sensitive to zinc restriction. When we restricted zinc, within eight to ten weeks, thymulin activity declined, even though there was no change in plasma zinc. Blood levels of zinc stayed normal for twenty-four weeks because we were restricting zinc slightly, but thymulin activity was affected; interleukin-2 was affected as well.
These findings indicate that the immunological functions are far more sensitive to zinc than anything that you can measure in the laboratory.
Regarding cognitive deficiencies, my colleague Professor Harold Sandstead did some work on Chinese dwarfs, and he found that they had impaired cognitive functions which were improved by zinc supplementation.
ZINC THERAPY FOR ACUTE DIARRHEA
We went through the first stage where we thought that zinc was not important for humans, then the second phase where we thought that deficiency was very rare. Now we know that zinc deficiency is common. And now we have learned that there are some very important therapeutic effects of zinc in certain conditions.
The first one has to do with infants and children in developing countries, where they frequently suffer from acute diarrhea and respiratory tract infections. I was invited to Bangladesh about twelve years ago, and I was shown a ward of one thousand babies with acute diarrhea. The physicians told me that ninety percent would die within three weeks. They were being given oral rehydration solution, which was developed almost thirty years ago for treatment of diarrhea, but this oral rehydration solution did not save their lives.
Professor Bob Black from Johns Hopkins University, became very interested in zinc; he said since zinc is essential perhaps we should add some zinc to the solution. He had his colleague Ken Brown and others set up a program in India, Bangladesh and Pakistan. Indeed, they found that once they added zinc to the oral rehydration solution, the children lived, and the mortality went down very dramatically. They published this important observation in several papers.
One interesting side story is that when Bill Gates was visiting Bangladesh, he was told the story that these children with the diarrhea would have died, but we are giving them zinc and with zinc they would live. He went to India and he heard the same story; he went to Pakistan and heard the same story; so he went back to Seattle and asked his foundation to contact a zinc expert.
I got a call from his foundation to advise him about zinc. I went to the foundation, and they were asking all kinds of questions as to why they should invest money in treatment of diarrhea with Bill Gates Foundation funds.
I told them that if you give twenty million dollars and go to twenty countries, you would save millions of kids, you would see the result very quickly. They bought the idea and they gave twenty million dollars, and studies were done in twenty different countries.
A reporter for Time magazine was visiting Africa, going from one village to another talking to families. The families would tell them that they lost four children but the fifth one was living because they received a small tablet of zinc. She published her article on zinc in Time magazine. Now WHO has a program in seventy countries where zinc is mandatory for treatment of acute diarrhea. Truly, zinc is a life-saving element.
WILSON’S DISEASE
Wilson’s disease is a fatal genetic disorder. Normally the disease expresses itself by the time you reach twenty, thirty or forty years, and copper accumulates in the liver, brain and the kidneys. The patients die by the time they reach forty or fifty years old. But we discovered that if you give them zinc, you can decrease the copper burden.
This was an accidental discovery. In sickle cell anemia you find zinc deficiency, and I was interested in giving zinc to decrease the sickling of the red cells because when the red cells sickle, they produce pain all over the body. They clog up the blood vessels and there’s a pain crisis. In order to reduce the copper burden, however, I had to give them 150 mg of zinc a day. At that level, we found that the copper went down. Only then do you see low serum copper, low ceruloplasmin and microcytosis (small red blood cells).
We published these finding in The Journal of the American Medical Association in 1978 or so, and this gave us the idea that perhaps in Wilson’s disease and similar genetic disorders, we could use zinc to decrease the copper burden.
Dr. Brewer, my colleague, has been working with this premise for twenty years; he’s following about three hundred patients all over the country. What he’s found is that zinc is a very effective mode of therapy for Wilson’s disease.
The FDA has approved zinc as a therapy for Wilson’s disease, which used to be fatal but now can be managed very well.
ZINC AND THE COMMON COLD
Now a bit about zinc and the common cold. In 1984, George Eby from Texas reported for the first time that if you take zinc acetate or zinc gluconate lozenges, you can decrease the severity and duration of the common cold. But between 1984 and 2000 many studies were carried out, and the subject remained controversial. Half the reports said it works, the other half said it doesn’t work.
I came into the picture in the year 2000, when I did two studies, one published in the Annals of Internal Medicine and the other in The Journal of Infectious Diseases.
There were a lot of problems with the previous studies. In the first place was that the salts they were using for zinc lozenges were not appropriate. You must have something where zinc is released properly in the mouth when you take it as a lozenge. We found that gluconate or acetate was the proper salt to use.
The second thing we found was that if you start within twenty-four hours of the onset of a cold―there are eight to ten symptoms, and if you have two symptoms you start immediately―the lozenges are effective, but if you wait three or four days after the cold starts, then zinc is no longer an effective mode of therapy, and the cold will last eight days.
The final thing that we found was that in the chemical formulation, a lot of lozenges on the market have citric acid and many other binders; all these binders prevent zinc from ionization and therefore render it unavailable for action.
If all these three factors are taken care of we found that zinc is very effective; it will reduce the duration of a cold by 50 percent and severity by 50 percent. Recently, a big Cochrane review on zinc for the common cold was published, and it was picked up by The New York Times and the Los Angeles Times among many others. The review confirmed our results that indeed zinc will be effective if all these precautions are taken.
Zinc works by decreasing the adhesion molecules where viruses attach. So it makes sense that zinc works in the early stages of a cold, but not later after the viruses have attached to adhesion molecules.
SICKLE CELL DISEASE
Sickle cell disease is a genetic disorder. It turns out that these patients hemolyze red cells at a higher-than-average rate. The hemoglobin is very rich in zinc so they lose all the zinc in their urine, and they becme very deficient. Zinc can be very helpful for the the treatment of sickle cell patients.
MACULAR DEGENERATION
As we get older, at least 50 percent will develop macular degeneration, and this causes blindness. The National Institutes of Health has been conducting a study on eye diseases and zinc and other antioxidants for the last ten years. It turns out zinc is very effective in the prevention of blindness and the progression of macular degeneration.
But most interestingly, they also observed that mortality was decreased in those subjects who were receiving zinc alone versus those who were receiving other vitamins and antioxidants.
CARBON MONOXIDE POISONING
In Russia, a zinc histidine compound called Acyizol is being used for carbon monoxide poisoning very effectively. In mining and related industries, people are already using zinc histidine for carbon monoxide poisoning in Russia.
ZINC IN THE ELDERLY
The elderly are prone to pneumonia and upper respiratory tract infection; the incidence is something like 5-6 per year. Our recent study has shown that by supplementing them with zinc, you reduce the incidence by 66 percent.
Zinc has three major effects on immunology. First, it affects cell-mediated immunity; second, it is an antioxidant; and third it works as an anti-inflammatory agent. Why are these observations so important? Because if you look at the current concept of many chronic diseases including atherosclerosis, cancer and some neuro- degenerative disorders, it is oxidative stress and chronic inflammation that are implicated in these conditions. I suspect that zinc may be very helpful as a preventive agent for these diseases.
ZINC AND ENZYMES
When I started my research I knew of only three enzymes that required zinc: carbonic anhydrase, carboxy peptidase and alcohol dehydrogenase. Today, we know of over three hundred enzymes that require zinc, and we know of two thousand zinc-dependent transcription factors that are involved in cell biology.
One example of a zinc-dependent enzyme is super oxide dismutase, which converts the super oxide into hydroxy ions. Zinc generates metallothionein, and this protein detoxifies hydroxylione. Zinc is also an inhibitor of NADPH oxidase, which is involved in generation of free radicals.
In the past ten years we have learned that zinc works like a molecular signal. Once zinc goes from outside to inside the cell, it takes part in phosphorylation of many of components and participates in very important roles in the cell biology.
THE ACCEPTANCE OF ZINC
From an ignored mineral, zinc has now become so important in fifty years that a new society of molecular zinc cell biology has been formed. It has one hundred fifty members internationally. Our last meeting was in Australia. More and more scientists are now interested in the study of zinc, and there is considerable research on this subject. No doubt we will be learning a lot more about zinc in the future.
SIDEBARS
DWARFISM DUE TO ZINC DEFICIENCY
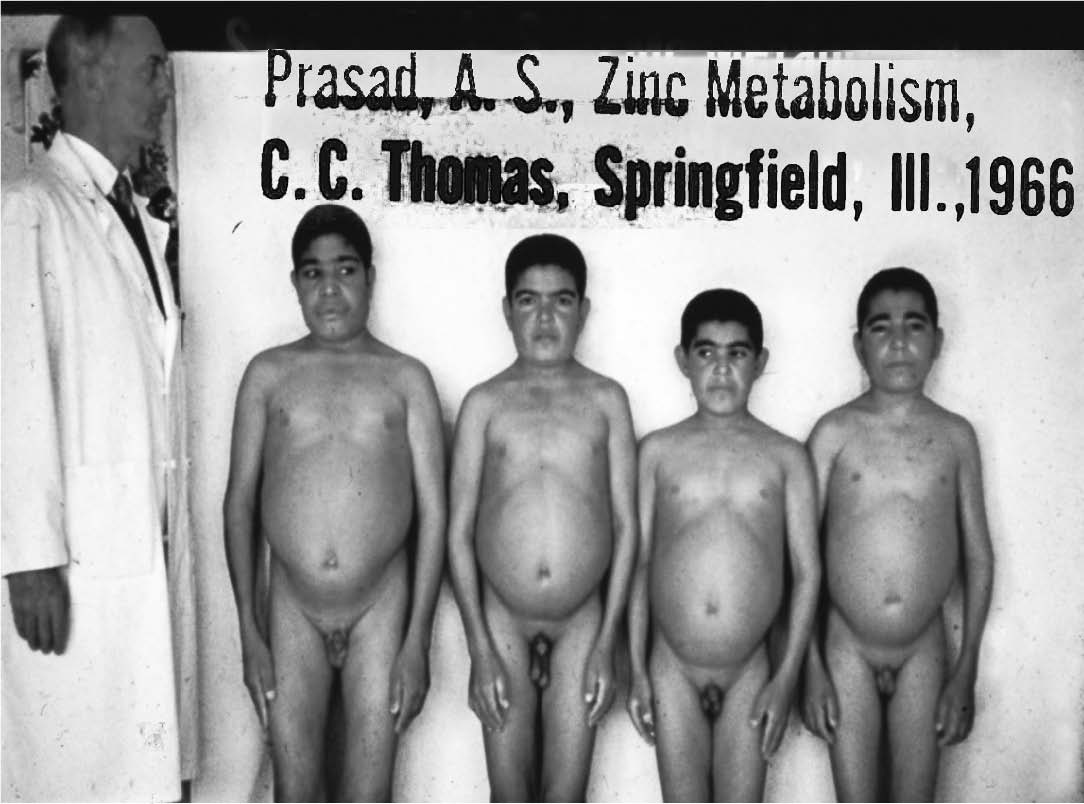
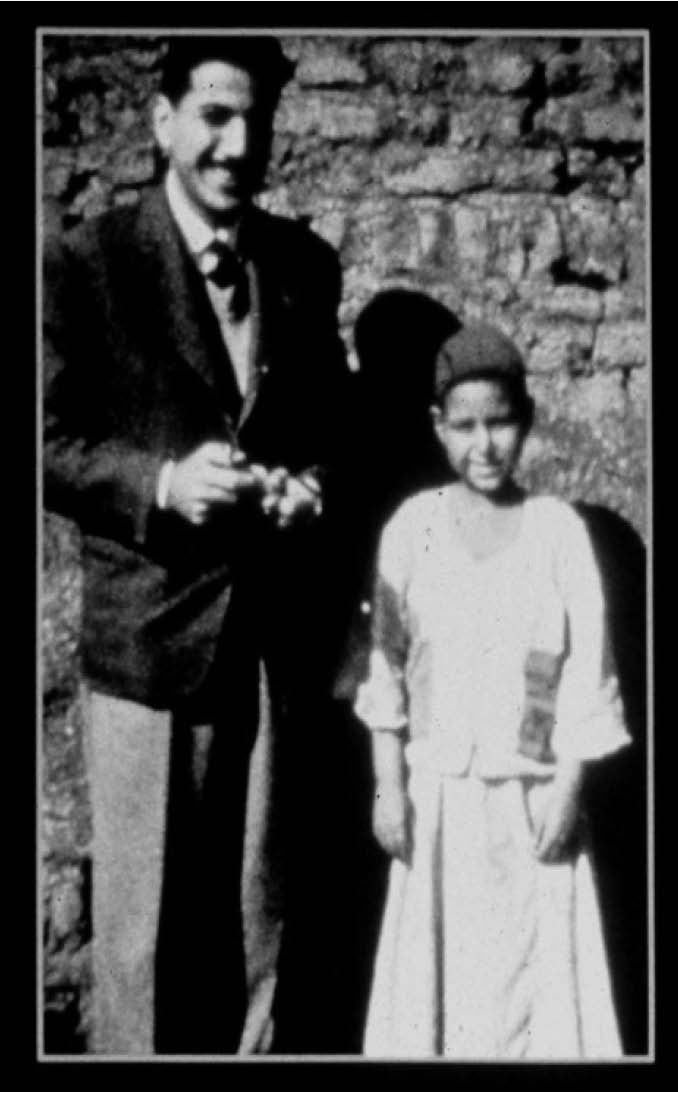
Severe zinc deficiency leads to dwarfism, hypogonadism and proneness to infection. Shown above, male dwarfs in Iran; to the right, a dwarf farm boy from an Egyptian village.
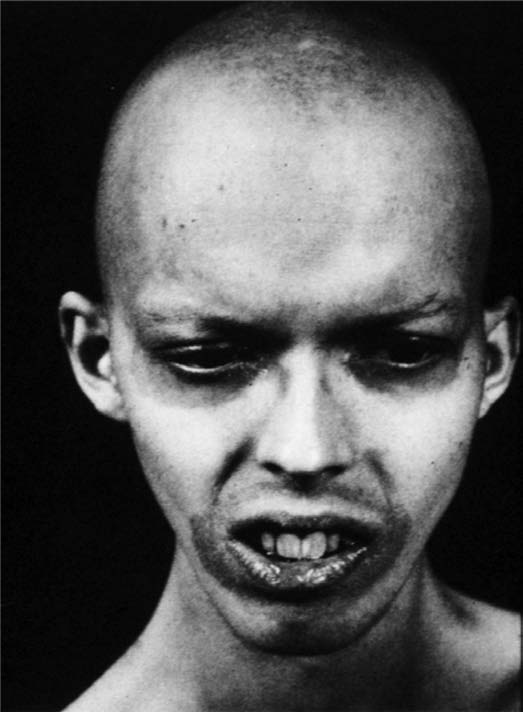
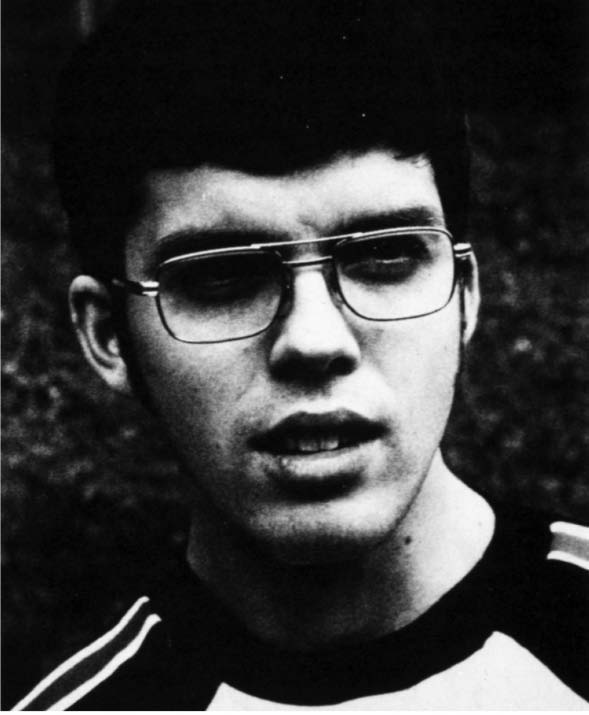
A CASE OF ZINC DEFICIENCY
This young patient with Wilson’s disease presents a
very severe example of zinc deficiency. The patient was
taking penicillamine to reduce toxic copper levels. He had
lost all his hair and had developed parakeratosis (a skin disease
characterized by dry, scaly skin) around his eyes and
mouth and in the axilla; his growth was affected and he
was also developing cognitive impairment. Analysis of zinc
levels in the plasma and in the red blood cells, in the urine
and the hair, showed the patient to be very zinc deficient.
Not only Wilson’s disease, but also the drug penicillamine,
contributed to the deficiency. Penicillamine is a chelator,
which chelates not only copper but also zinc. Once the
patient was given zinc, he had a complete recovery within
a few months; he even went to college.

This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly journal of the Weston A. Price Foundation, Winter 2012.
🖨️ Print post
Thank you for your research and this very informative article. Could you please tell me the dosages you used? Is there a toxic level? Or did you start with a low dose and increase as you saw fit? According to Sherry Rogers, M.D., Zinc Balance by Jarrow takes care of the copper problem when you take zinc. Last year in Oct., I started taking this zinc and have not had any colds/flu. A concern I have is that you can throw off other minerals by increasing one or two. I am still trying to understand that.
Wow! Think of all the lives you have saved. Extraordinarily wonderful! Thank you!
Thank you, Dr. Prasad, for your wonderful work on zinc deficiency.
Yes, I have to applaud you on a discovery that could help millions – some things, such as your invitation to go to Iran are meant to be. Congratulations for a job very well done!
I can empathize with your frustrations and tension at not being believed and having to struggle against colleagues.
Although my story does not have the magnitude of yours, I am a Canadian emergency physician who has discovered various forms of hypothyroidism and the factors that contribute to these forms – that is how I came across your wonderful story. I strongly feel that discovery of these hypothyroid conditions could prevent dementia, Parkinson-type syndromes, CHF, arrhythmias, myocardial infarctions, extreme muscle weakness, and, a host of disabling conditions. My colleagues criticize me for unnecessary testing, and, limit my clinical investigations.
Perhaps, it was no accident that I happened across your article.
Thank you, once again.
Ron Matsusaki
Digby General Hospital
Digby, Nova Scotia B0V 1A0
1-902-245-2502 Ext 3229
Dear Dr. Matsusaki.
I salute you for the bravery and dedication.
I am 85 yrs age. I had cancer of the upper right septum 15 years ago and suffered periodic nasal bleeding as a result though my cancer was, and has been,in remission. My tissue was super sensitive and provided excesses of phlegm. I have taken brewed saffron tea for the past 2 years which provided some relief and revitalization of skin tissue though remaining quite sensitive when irrigating my nasal passage with salt and warm water. Recently I began suffering extreme discahrges of phlem with quantities of blood. The Doctor thought it sinus related and nothing serious and perhaps due to a recent chest flu condition with coughing and phlegm discharges and a few days of bed restricted fever(102)conditions and rest. However, though bleeding was lessened as fevers declined, Sinus discharge with some blood continued. I chanced to catch sight of a comment in a Google search as to zinc deficiency being a possible contributing factor. I need to mention I have had cronic lower colon aches and diarrhea for many years so that it has become an accepted never-to-go-away condition. I recollected I had secreted away in an upper pantry shelf an ancient unused bottle of Chelated Zinc 25mg. On a whim I decided to try the zinc tablets for a few days. For the first time in 50 years my diarrhea has been greatly reduced and almost vanquished. My sensitive nasal tissues are toughened and regenerated. I have no bleeding condition, sinus or otherwise. My taste bud sensitivity seems to have increased and impacted my appetite in a positive manner. Over the years i’ve had tests for vitamin deficiencies, blood tests, allergiy tests, et al and no one ever tested me for a zinc deficiency. I am a convert. If anyone has ANY ailment and you’re up in years i recommend you try a few days of zinc and see what, if anything, happens. For myself i will take zinc from now and until the end.
FG
Thank you. The article is very informative. Could you advice me where I could get a good quality oyster extract because I heard it is a good source of zinc supplement? A.L.
Dr Prasad, your work for this article is fantastic.
Would you recommend a good Zinc Supplement, if I am not able to consume enough in my normal diet?
Dr. Prasad, Do you think zinc helpful in autoimmune disorder, Is there is any connection between zinc, thymus and autoimmune disorder?
Estive na Bélgica, uma semana até 10 Fevereiro. Levei comigo como prevenção para o Covid, o Gluconato de Zinco. Valeu. Eu nem sabia bem os sintomas do Covid-19, mas quando a mim e minha esposa, nos faltaram o cheiro em cima das dores musculares, irritação da garganta… percebi. Eih! …é ele! E em 3 dias a 50 mgr e depois 25 mgr e óleo de fígado de bacalhau, tudo desapareceu antes de uma semana.
‘ Só ‘ tenho 73 anos e em tempos colocaram-me
6 stent expansores das coronárias… Depois de outra ‘descoberta’, com magnésio e sem droga alguma, vivo com o colesterol a 254, faz 3 anos. Dr. Ananda Prasad, se precisar de um lugar no céu… ‘eu arranjo!’ Obrigado!
Que bom ver um português no este site). Bem haja!