






Weston Price was far more than a dentist.
He conducted his pioneering work in nutritional and medical anthropology, which culminated in his epic treatise, Nutrition and Physical Degeneration,1 after twenty-five years of laboratory and clinical research into the causes and consequences of tooth decay had already earned him national recognition as a leading scientist. The work contained therein is far more than an interesting travelogue or a survey of the health of traditional cultures: Price recorded within its pages nature’s closest approximation to the gold standard of today’s evidence-based medicine, the randomized controlled trial.
The Scientific Background
In 1915, Price became the first director of the American Dental Association’s Research Institute.2 By that time, he had been administrating his extensive research program for fifteen years and had already published over one hundred fifty papers in scientific journals. As director of the Research Institute, he led a team of sixty scientists and had at his disposal an advisory board of eighteen of the leading scientists in a variety of disciplines, including Victor Vaughn, then president of the American Medical Association, and Charles Mayo, a founder of the Mayo Clinic.
Several of Price’s findings from these early studies formed the foundation of the research he later published in Nutrition and Physical Degeneration. He had found it difficult to induce tooth decay in animals simply by introducing a putative cause and concluded that susceptibility to tooth decay likely involved a deficiency of protective factors. Price could distinguish animals and humans who were susceptible to tooth decay from those who were immune simply by measuring whether their saliva extracted or donated minerals when he mixed it with powdered bone: saliva from immune individuals always donated minerals to the bone.
Price’s twenty-five-year research program, however, was unable to answer a critical question: what were the protective factors that provided this immunity? To answer this question, Price turned to other cultures with populationwide immunity to tooth decay.
Price’s Study Design
Price understood the need for scientific controls, and Americans without tooth decay at that time were a rarity. He also wanted to establish “standards of excellence” to see just what sort of freedom from physical degeneration was possible. Emphasizing the need for scientific controls, he set out not simply to observe foreign people free of tooth decay, but rather to observe both immune and susceptible groups who could be closely matched for heredity, culture, latitude, altitude and climate. Thus, he looked specifically for genetically homogeneous groups on the cusp of modernization to serve as a series of what we could call “natural experiments.” (See Figure 1.)
FIGURE 1: A SERIES OF NATURAL EXPERIMENTS
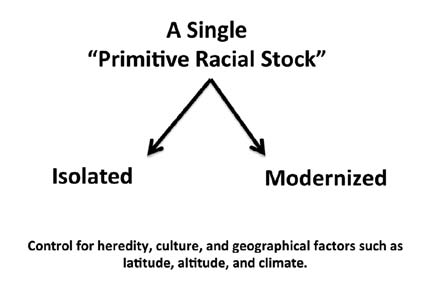 Price sought out “primitive racial stocks,” by which I believe he meant genetically homogeneous groups that were “primitive” both in the sense that they had not yet modernized and also in that they had not mixed with other races, since a common theory at the time was that dental deformities were caused by race mixing. Wherever he could, he studied these groups on the cusp of modernization so that he could find some subgroups that had remained “isolated” from modernizing forces and others that had already modernized or that were in the process of modernizing. This allowed him to control for factors that were relatively homogeneous within each “primitive racial stock” but radically different between “primitive racial stocks.” Ordinarily, these factors confound observational studies and make their results difficult to interpret. Experimental studies attempt to control for them through randomization. Controlling for them in this unique way rendered Price’s observations similar to a series of “natural experiments”—observations of the results of, as Price put it, “Nature’s great biological laboratory.”
Price sought out “primitive racial stocks,” by which I believe he meant genetically homogeneous groups that were “primitive” both in the sense that they had not yet modernized and also in that they had not mixed with other races, since a common theory at the time was that dental deformities were caused by race mixing. Wherever he could, he studied these groups on the cusp of modernization so that he could find some subgroups that had remained “isolated” from modernizing forces and others that had already modernized or that were in the process of modernizing. This allowed him to control for factors that were relatively homogeneous within each “primitive racial stock” but radically different between “primitive racial stocks.” Ordinarily, these factors confound observational studies and make their results difficult to interpret. Experimental studies attempt to control for them through randomization. Controlling for them in this unique way rendered Price’s observations similar to a series of “natural experiments”—observations of the results of, as Price put it, “Nature’s great biological laboratory.”
By showing that physical degeneration followed the adoption of “the displacing foods of modern commerce” in each modernized group while each group that remained true to its traditional diet remained free of degeneration, Price showed that these effects were not a result of factors that could have confounded a comparison between groups, such as heredity, culture or geography. By showing that this trend persisted in so many different groups regardless of these factors, Price showed that the effect was robust and independent of them.
Price described his search in this way (page 472): “A comprehensive study of modern degeneration will require the use of controls in order that standards of excellence may be established. Not finding adequate controls in our affected groups, it became necessary to look elsewhere in Nature’s great biological laboratory, which has been in operation throughout the history of life.”
Price performed dental examinations, took thousands of pictures, collected dietary and other ethnographic information, and collected samples of food, soil, and saliva for laboratory analysis. Had Price used these extensive data simply to compare one group to another, his conclusions would have been riddled with problems (see Sidebar). Price’s unique study design, however, allowed him to do something quite different: he made all of his comparisons between the isolated and modernized subgroups of each culture. By comparing the isolated Swiss to the modernized Swiss, and the isolated Gaelics to the modernized Gaelics, and so on, Price made comparisons wherein both isolated and modernized subgroups of each culture had similar genetics, a similar cultural history, and lived in similar climates and at similar altitudes and latitudes.
Nature’s Randomized Controlled Trial
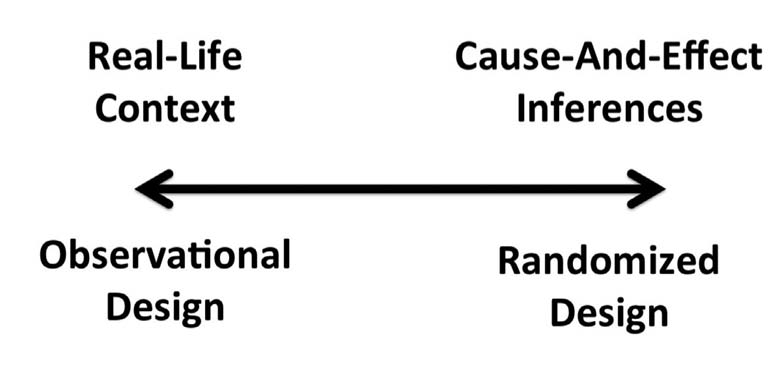
Price’s unique approach allowed him to maximize both the real-world context of his work and his ability to make inferences about cause and effect, which are two qualities of scientific research that are ordinarily at odds with one another (See Figure 2).
FIGURE 2: THE SCIENTIFIC TRADE-OFF BETWEEN OBSERVATIONAL AND RANDOMIZED DESIGNS
The types of evidence we use to study human health generally fall into two types: observational and randomized studies. In observational studies, scientists observe things the way they are, without experimentally manipulating anything. In randomized studies, scientists randomly allocate whatever or whomever they are studying—whether chemicals, cells, animals or humans—to different groups receiving different experimental treatments. The strength of observational studies is that the context is much closer to the day-to-day reality of most people, while their weakness is their lack of control for factors that confound our ability to infer cause-and-effect relationships. Conversely, the strength of randomized studies is that they control for these confounders, but their weakness is that they lose real-world context. The more rigorously we control a system, the more we distort it. And, the more we know how that distorted system works. Any evidence thus falls somewhere on the spectrum shown below. Yet the trade-off isn’t a zero-sum game. Scientists usually work with highly distorted yet very knowable experimental systems, always searching for ways to maximize the relevance of these systems so that their amenability to being studied isn’t all for naught.
Within any population, we can expect to find a distribution of many different factors that could influence the risk of disease. These include differences in diet, lifestyle, and hereditary factors such as genetics. If we simply observe how these factors correlate with health and disease, whether we are comparing individuals within a population or comparing one population to another, this multitude of potentially important factors makes it extremely difficult to understand cause-and-effect relationships. Because these factors make the interpretation difficult, we call them “confounders.”
In order to make a strong inference about cause and effect when we observe a difference between two groups, we want the distribution of potential confounders to be as close to identical as possible between them. The only reliable way to do this is to randomly distribute participants into each group. Because the means of allocating participants to a group is random, every single potential confounder—even if it is a confounder that no one knows about or has even imagined— has an equal chance of winding up in each group. For this reason, scientists consider the randomized controlled trial to be the most reliable means of studying cause-and-effect relationships in humans.
The effectiveness of randomization is proportional to the number of participants in a study. Imagine flipping a coin: if you flipped a coin twice, you would not necessarily get heads once and tails the other time. If you flipped a coin several hundred times, however, you would likely get heads very close to half the time. Even very large randomized controlled trials, however, have limitations: they are usually far too short to understand the long-term effects of anything, and they are always conducted in a dramatically different context than anything we could call “real life.” At a minimum, researchers are monitoring the subjects and telling them what to do, which puts the subjects in a different category than people acting spontaneously. The scientists are likely drawing their blood, which in and of itself affects a person’s biology (most obviously by removing iron and red blood cells), and in extreme cases they may be locking the subjects in metabolic wards under close surveillance and even controlling their physical activity. As a result, randomized controlled trials gain the ability to make inferences about cause and effect at the expense of real-world context (Figure 2).
The communities Price studied were likely much more homogeneous than our own modern society, with its ethnic melting pots and vast proliferation of choices. They nevertheless undoubtedly had their own distributions of dietary, lifestyle and hereditary factors. Although the distributions are unlikely to have been identical from, for example, one Swiss village to the next, they are likely to have been quite similar. Indeed, they are likely to have been far more similar between two Swiss villages than they would have been between a Swiss village and an African tribe, or between obese Americans with heart disease and lean Americans with healthy hearts.
Price’s study design thus targeted the best of both worlds. It was observational, and firmly rooted in real-life context, free of experimental controls. At the same time, he exploited an opportunity that was largely unique to the brief window of time open to him, wherein so many different groups were on the cusp of modernization all over the globe. Thus he had the opportunity to make repeated observations in many different geographical, cultural and genetic contexts, wherein he could compare isolated and modernized groups with as similar distributions of confounding factors as possible. While this is not, overall, the most effective way to remove factors that confound inferences of cause and effect, it is the most effective way to do so in an entirely natural and spontaneous context. Few other studies could get the best of both worlds in this way, and probably none has ever done so on such large a scale.
In this sense, Price’s study design was to observe the closest thing to a randomized controlled trial that nature has to offer.
Price’s Central Finding
Price found that the most consistent change that occurred with modernization was the replacement of traditional diets with the “displacing foods of modern commerce.” These foods, according to Price, included white sugar, white flour, white rice, syrups, jams, canned goods, and vegetable oils.
Price verified in the laboratory that the nutrient contents of soil and individual foods were also much higher among the traditionally living groups, and that their saliva donated minerals to powdered bone, a characteristic he had long associated with immunity to tooth decay. In every instance, modernization was associated with a proliferation of tooth decay in the first generation and dental deformities in the second. Attributing the disease to the dietary changes is not completely free of confounding, but the finding was robust across so many cultures and genetic stocks in so many different latitudes, altitudes, and even continents, that we can conclude that the risk of confounding is extremely low.
The Scope of Price’s Work
Although Price’s central finding focused on a decline in dental health, his work is broader than this. He provided evidence that tuberculosis, cancer, ulcers, appendicitis, cystitis, and gall bladder disease also increased, with the evidence being strongest for tuberculosis. He also performed animal experiments and clinical interventions, provided fascinating anecdotes from his clinical experience, and set his research in the context of the most rigorous science of the time, which together offered even stronger support for his hypothesis that nutritional deficiencies induced by the “displacing foods of modern commerce” were behind these epidemics of degenerative disease.
One of the most impressive things about the scope of Price’s investigations is the sheer amount of data he collected. By 1929, for example, Price had already been taking samples of butter between once a month and once a week from two hundred seventy locations in the United States, Canada, Cuba and Mexico to measure the vitamin content Along with these samples, he collected additional information about the date the animals were milked as well as their diets and living conditions. By 1945, Price had analyzed over twenty thousand samples of butter and had expanded the operation to include locations in Australia, Brazil and New Zealand. He also mentioned measuring the vitamin content of butter samples from Switzerland and Egypt. With these data, Price showed that even in a single location, the vitamin content in dairy products could vary up to fifty-fold seasonally, and that in sixteen different regions the fluctuation in vitamin content over the course of the year was inversely related to the mortality from heart disease and pneumonia.
Price demonstrated among his own patients that the simple addition of high-vitamin butter oil and cod liver oil could alter the properties of saliva in a way that favored immunity to the tooth decay. He also performed controlled animal experiments showing that rats grown on whole wheat were immune to tooth decay, while those grown either on white flour or bran were highly susceptible. He conducted other experiments in rats and turkeys showing that high-vitamin butter oil and cod liver oil synergized to promote healthy mineral balance, protecting against rickets and weak legs.
Price conducted a nutritional intervention in his patients consisting of the following: three-fourths teaspoon each of high-vitamin butter oil and cod liver oil chased with four ounces of tomato or orange juice; stews made from green vegetables, carrots, meat, marrow, and the juices of broiled meat, which were rotated with organ meats and fish chowder; rolls made from freshly ground wheat with liberal quantities of high-vitamin butter; cooked fruit; and two glasses of whole milk. This regimen reversed over 90 percent of active cavities, without the need for fillings, as shown by X-rays and in limited cases by silver nitrate staining.
Although Price did not have a control group, his findings are consistent with those of a controlled study based on similar principles published by May Mellanby, who discovered vitamin D with her husband, Sir Edward Mellanby.4 Price also cited a controlled study showing that cod liver oil reduced the incidence of tooth decay. The findings are simply remarkable, moreover, and the likelihood of such a reversal occurring by chance seems negligible.
Price’s work went beyond dental health. His evidence that modernization led to a dramatic increase in the risk of tuberculosis included the following:
- Although the Swiss government considered tuberculosis the most serious disease affecting Switzerland, Price found not a single case among the isolated groups of the Loetschental Valley. Several Swiss clinicians told Price that tooth decay tended to correlate with tuberculosis among the modernized Swiss.
- On the Isle of Lewis, tuberculosis was rapidly becoming a problem in the younger generation inhabiting the modernized parts of the island, despite the immunity of previous generations.
- Price was unable to find people living under primitive conditions in Wales. Some suggested he might find such people on the Island of Bardsey off the northwest coast, but the people he found living there were recent colonists living largely off white flour, marmalade, sugar, jam and canned goods. Tuberculosis, mouth breathing, and tooth decay were rampant. Public health officials told Price they believed that the people’s defenses against the disease were declining for unknown reasons. Like the Swiss investigators, they observed a tendency for tuberculosis and tooth decay to correlate. To Price, the walls of the ancient castles, cemeteries, and great monuments of this island bespoke the glory and power of a lost people. In the new era, tuberculosis had wiped out the people almost to the point of extinction. The government had recently repopulated the island with fifty healthy families, but they too were dying of tuberculosis.
- Similarly Price found severe cases of tuberculosis among the modernized North American Indians, but did not report any cases among the traditional subgroups, noting that the “modernized Indian children are dying of tuberculosis which seldom kills the primitives.” Price was also able to find some Indians at the point of contact with modern civilization where tuberculosis appeared to attack the younger generation whose bodies were built on modern foods, with the typical signs of modernization such as mouth-breathing, dental deformities and an underdeveloped middle third of the face, whereas the parental generation appeared to be free of the disease. He made similar findings among the native Alaskans. Finally, he also spoke to Dr. Josef Romig, a surgeon with thirty-six years of experience among both traditional and modernized subgroups, who told him that large numbers of modernized natives of Alaska and Canada die of tuberculosis. The good doctor told them to return to their traditional diets, on which they tended to recover.
- Price also found tuberculosis common among the modernized groups of Peru, the Pacific Islands, Africa, and Australia.
- In some cases, Price examined the rates of dental deformities in tuberculosis sanataria, such as those in New Zealand and those housing modern Americans, and found rates exceeding 90 percent and even approaching 100 percent.
- The native Maori considered the traditional seafoods, particularly fish organs, as highly effective in the treatment of tuberculosis, indicating they had some experience with the disease, but were apparently able to keep it in check with good nutrition.
- Finally, Price cited published research conducted among modern Americans showing a strong statistical relationship between an underdeveloped, deep, narrow chest, rather than a “flat and wide” chest, and tuberculosis. These also correlated with low income. While Price recognized the role of bacteria in the disease, and the role of nutrition in the immune defense, he considered poor nutrition during development to make a major contribution to the increased risk of tuberculosis among modernized people by compromising the development of the chest cavity just as it compromises the development of the face and dental arch.
- It is possible that isolation could have protected many of these groups from the spread of the tuberculosis bacterium, but nutrition almost certainly played its own role. Price provided limited evidence, moreover, that other diseases were associated with modernization. This evidence includes the following:
- Dr. Romig, mentioned above, informed him that in thirty-six years of experience treating both primitive and modernized natives of Alaska and Canada, he had never seen a single case of malignancy among the primitives but found it frequently among those who had modernized. Similarly, acute surgical problems with internal organs such as the gall bladder, kidney, stomach, and appendix were rare among the primitives and common among those who had modernized.
- Dr. J. R. Nimmo, the government physician serving a group of Torres Strait Islanders for thirteen years, informed Price that he had operated on several dozen malignancies in several hundred modernized whites over the course of that time, but had not seen a single definite case and had seen only one possible case among some four thousand traditionally living natives over the same period. Nimmo also stated that other issues requiring surgical intervention were rare among these natives.
- Dr. Andersen, in charge of a government hospital in Kenya, informed Price that in several years serving the primitives of that district he had rarely seen malignancies and had seen no cases of appendicitis, gall bladder trouble, cystitis, and duodenal ulcer.
- Price also provided fascinating anecdotes from his clinical experience, wherein nutrient-dense foods corrected seizures and chronic fatigue related to low blood levels of calcium, and made remarkable improvements in childrens’ performance at school. He even performed a surgical intervention to correct a narrowed palate that induced puberty in a child long failing to develop through that stage of life, probably by releasing pressure on the pituitary gland.Thus, while Price’s most rigorous findings were those falling within his field of specialty, oral health and dental deformities, he also made a compelling case that the “physical degeneration” associated with modern refined foods is much broader in scope, and that adequate nutrition beginning with the prenatal nutrition of the parents and continuing through development and adulthood is one of the most importance defenses we have against disease, and one of the most important bulwarks we have to support vibrant health.
Primitive Wisdom
One of Price’s central conclusions, as described in more detail in the Fall, 2011 issue of this journal, was that the traditional cultures he studied successfully maintained vibrant health on their traditional diets not by accident, but because they had accumulated wisdom about how to nourish their soil, plants and animals, and thereby nourish themselves. This quote (page 161) captures his conclusion well:
“In my studies of these several racial stocks I find that it is not accident but accumulated wisdom regarding food that lies behind their physical excellence and freedom from our modern degenerative processes, and, further, that on various sides of our world the primitive people know many of the things that are essential for life—things that our modern civilizations apparently do not know. These are the fundamental truths of life that have put them in harmony with Nature through obeying her nutritional laws.”
It may be tempting to suggest that Price’s studies of hunter-gatherers offer insight into our “evolutionary past” and even the superiority of “evolutionary diets” devoid of cereal grains. Price did offer an evolutionary perspective, which is discussed in more detail in the sidebar on page 22, but his purpose in studying huntergatherers was the same as his purpose in studying horticulturalists, pastoralists and agriculturalists: not to develop windows into the ancient past, but rather to study “standards of excellence” in a rigorously controlled manner.
As discussed in the sidebar below, Price’s data offer little if any support to the belief that cereal grains are unhealthy. On the contrary, Price concluded that some groups were able to successfully use cereal grains to support vibrant health because they had accumulated the wisdom necessary to do so.
Modern Knowledge
In Price’s assessment, the mistake of modernity was to emphasize the accumulation of knowledge at the expense of wisdom (page 301): “There are two programs now available for meeting the dental caries problem. One is to know first in detail all the physical and chemical factors involved and then proceed. The other is to know how to prevent the disease as the primitives have shown and then proceed. The former is largely the practice of the moderns. The latter is the program suggested by these investigations.”
Price was not against learning “in detail all the physical and chemical factors involved,” and in fact he devoted considerable effort to learning about these factors. His opposition here is to insisting on completing this knowledge first, before proceeding to address the problem of modern degeneration by tapping into the solutions found among the successful “primitive” groups he studied.
Price observed the backward steps that modern society kept taking with each new piece of knowledge it obtained. With a little knowledge, it first removed the vitamins from its bread. With a little more, it replaced these with isolated vitamins. Price cited a study showing that isolated vitamin D caused placental calcification and fetal kidney stones when given to pregnant women, whereas cod liver oil did not. After seeing the tooth decay that resulted from white flour and sugar and the soft tissue calcification that resulted from pure vitamin D, how could Price be anything but discouraged by the track record that the progress of knowledge had generated?
The problem was that many, once they obtained some new knowledge, were tempted to sacrifice the wisdom of previous generations rather than use their knowledge to further enrich the pool of accumulated wisdom. Price was humble enough to learn from the Swiss, who “recognize the superior quality of their June butter, and without knowing exactly why, pay it due homage.” Others would simply discard this recognition because it was not rooted in the superior epistemology of modern science, considering it perhaps even worthless precisely because the Swiss paid this homage “without knowing exactly why.”
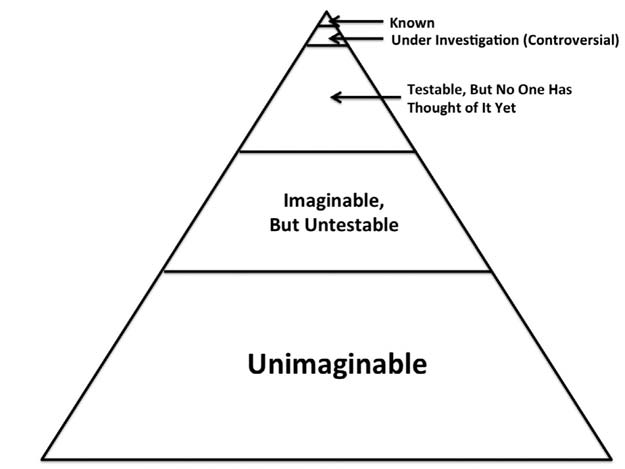
Price strongly advocated the humble sentiment that what we do not know likely far exceeds what we do know. Indeed, it may be that what we know is only the tip of the iceberg (Figure 3). He used this sentiment to justify his continual support for the use of natural foods, which may differ from modern substitutes in ways we do not completely understand. “Great harm is done, in my judgment,” he wrote, “by the sale and use of substitutes for natural foods” (page 294).
Placing Price’s Work in Context
Tradition, of course, has its limitations. It would be just as problematic to discard the scientific method and blindly accept every human tradition as it would be to discard the wisdom of past generations. It would be similarly problematic to discard our own experience in deference to either of these sources of knowledge. How are we to respect and embrace the wisdom of our ancestors, while using science and our personal experience to refine and enrich the pool of accumulated wisdom?
In other words, how are we to place Price’s work in its proper context?
There are many legitimate uses of evidence, some of which are as simple as collecting observations about the world for the sake of curiosity and appreciation. Evidence that should inform our decisions about how to eat and live to be healthy could be broadly divided into three categories, each of which makes its own essential contribution: evidence supporting a framework for interpreting how to act in the face of uncertainty, experimental evidence demonstrating cause-and-effect relationships, and personal experience.
FIGURE 3: THE GREAT UNKNOWN
Price placed a strong emphasis on acknowledging the things we do not know. As shown above, we might suppose that most of what is true probably is not known, the bulk of which is likely untestable or unimaginable. Although not shown, much of what is “known” may be wrong.
The modern program that Price opposed, which was to “know first in detail all the physical and chemical factors involved and then proceed,” superficially appeared to be based on scientific certainty. In reality, however, it took the status quo as its framework for interpreting uncertainty. Refined flour and sugar were the norm, and society’s managers added nutrients back to the diet one by one as science demonstrated their importance. Price argued for a “common sense” that took for granted diets associated with health rather than those associated with disease. In other words, a “common sense” rooted in evidence rather than in the status quo.
Price documented a broad range of traditional diets that were consistent with freedom from disease at a population level, meaning even the most vulnerable members of the population were protected. We may not be able to say with certainty that every single element of every single traditional diet is health-promoting, but we can certainly say that this range of traditional diets is consistent with population-wide freedom from disease. Thus, this range offers a much better source of “common sense” about diet than the current status quo.
Price provided strong evidence that the transition from diets based on traditional, nutrientdense foods to diets based on the “displacing foods of modern commerce” caused the physical degeneration that ensued. Thus, the central theme of our approach to nutrition should be to emphasize nutrient-dense foods and banish refined foods and vegetable oils.
While this finding is incredibly powerful in itself, it leaves much to be answered. Were some traditional diets superior to others?5 Were certain factors protective rather than others? Were some neutral, or some harmful? How do they work together in the proper balance? What is the full range of diseases attributable to diet?
For diseases that are less clearly attributable entirely to the nutritional transition, such as heart disease, what are the roles of sleep, stress, social structure, infection and other variables? How do all these factors interact with features unique to our own society? Do our modern lives place special demands on us?
We can broaden, deepen and strengthen our understanding of Price’s work with experimental science, through which we can begin to provide answers to some of these questions. Valuable experimental evidence ranges from experimental animal and cell models that deepen our understanding of physiology to randomized, controlled, clinical trials in humans that provide clear evidence for effects on human health.
Each individual, finally, is unique and dynamic. As a result, one person’s nutritional needs may differ from another’s, and her needs at one time in her life may differ from her needs at another time. Even after all the foregoing evidence is taken into account, then, a person must heed her own experience.
The work of Price and others following his approach thus lays our foundation of common sense, while experimental science broadens and deepens our understanding of how to achieve health, and our personal experience fine-tunes our approach to an individual level best suited to each of us. In this way, we seek knowledge not to replace the wisdom accumulated by our ancestors, but to build upon, expand, refine and enrich this pool of accumulated wisdom.
SIDEBARS
COMPARING DIFFERENT TRADITIONAL CULTURES IS FRAUGHT WITH PROBLEMS
Price’s approach was to compare isolated and modernized subgroups within each of the cultures he studied. It may be tempting to use his data to compare one traditional culture to another, but this is a far less valuable and far more confounded approach. To illustrate why, let us consider how adaptations in vitamin D metabolism among the Inuit could confound such a comparison between this group and any of the others Price studied.
Suppose we compared the Inuit and the Gaels. On page 441 of Nutrition and Physical Degeneration, we see that the traditionally living Inuit had only 0.09 percent of teeth attacked by cavities while the traditionally living Gaels had 1.2 percent of teeth attacked. Thus, the Gaels had thirteen times more tooth decay than the Inuit. We might conclude from this that the traditional Inuit diet is superior to the traditional Gaelic diet, perhaps because it did not contain oats or other cereal grains.
Such a conclusion would ignore the fact that the Inuit and Gaels might have hereditary differences that affect skeletal and dental health. In fact, there are good reasons to believe that the Inuit have specific adaptations related to vitamin D metabolism that protect their skeletal health at the expense of other measures of health, particularly the nervous system.
Explorers have long described a phenomenon called pibloktoq, a form of hysteria, among the Inuit of the Thule District of northern Greenland. There is considerable evidence the phenomenon could result from low blood levels of calcium during times when vitamin D and calcium are scarce:6
• The disorder involves a period of hours or days in which the person seems irritable or withdrawn, followed by sudden, wild excitement with irrational, offensive, and dangerous behavior. It ends with convulsions and stupor. Finally, the person recovers but cannot remember the experience.
• It certainly occurs in northwest Greenland, probably occurs elsewhere in Greenland, and might occur anywhere in the world. The degree to which it is a specifically Inuit disorder is unclear.
• It occurs most often in the late winter and early spring, and least often in the summer.
• It can reach epidemic proportions in the Thule district.7
• It resembles tetany, a condition caused by low concentrations of calcium in the blood, which involves involuntary muscle spasms and sometimes severe convulsions, and is often complicated by emotional and cognitive disorganization.
• Medical reports have often noted a tendency towards signs of tetany, such as convulsions in infants and leg cramps in adults, among the Inuit.
• In certain regions of Alaska and Greenland where the fishing is poor, access to calcium from dried whole fish and vitamin D from marine oils is often scarce. Combined with lower availability of vitamin D from sunlight, whether because of latitude or clothing, Inuit dwelling in these regions could easily become deficient in vitamin D and calcium, especially during the winter.
• In someone already suffering from low total calcium, prolonged deep breathing or hyperventilation from emotional stress could lower the concentration of carbon dioxide in the blood, which would in turn alter the acid-base balance and thereby reduce the concentration of ionized calcium in the blood. Thus, the ionized calcium would transiently become low enough to cause an attack.
There is just one problem with this argument: if the Inuit are vulnerable to tetany caused by vitamin D and calcium deficiency, why have rickets and osteomalacia been so rare among them? One author suggested that the physically difficult Arctic environment led to adaptations in vitamin D metabolism that spare the skeleton at the expense of the nervous system by reducing the normal blood concentrations of parathyroid hormone.3
This explanation is quite plausible. Calcitriol, the most active form of vitamin D, will increase the amount of calcium we absorb from food all by its own, but it needs the help of parathyroid hormone to leach calcium from the bones so that it will enter the blood and become available to the nervous system. As a result, parathyroid hormone helps spare calcium for the nervous system at the expense of the skeletal system. Conversely, a lower level of parathyroid hormone would spare calcium for the skeletal system at the expense of the nervous system.
A 2004 paper published in Calcified Tissue International supports this idea. Inuit consuming “western fare” and living in Denmark had lower 25(OH)D, a marker of vitamin D status, than Danes. They had higher calcitriol, however, and lower parathyroid hormone. Inuit consuming “traditional fare” had 25(OH)D levels comparable to Danes, but had even higher calcitriol and even lower parathyroid hormone. Thus, the Inuit seem to have specific adaptations that allow them to produce high levels of the most active form of vitamin D, along with low levels of parathyroid hormone, even when vitamin D is relatively scarce. In such times of scarcity, we would expect this adaptation to support their skeletal systems at the expense of their nervous systems.
Price’s data is consistent with this hypothesis. The Inuit not only had one of the lowest rates of tooth decay on their traditional diet; they also had one of the lowest rates of tooth decay on a modernized diet: only 13 percent, compared to thirty percent among the Gaels and Swiss.
This is just one illustration of hereditary differences in skeletal metabolism that could exist between the different traditional cultures that Price studied. There are likely many other examples, making it important to emphasize Price’s intentional study design—comparing isolated and modernized subgroups of each culture—over the many other much more confounded observations we could casually make when reading his work.
PRICE’S EVOLUTIONARY APPROACH
Although Price did not study hunter-gatherers as windows into our evolutionary past, he did write about the importance of understanding biological evolution in the 1945 edition of his book, in the chapter entitled “How Mother Nature Made Us.” There he wrote the following (pages 460-1):
“It is exceedingly important that if we are to stem the tide of modernized self-destruction, that we come to know the nature of and origin of both our physical being and our personalities, in order to ascertain what we have lost and how the loss may be prevented. As an approach to this it is important that we review and visualize our origin. The current teachings of the three R’s and simpler sciences and most of our religious and social philosophies have failed to relate us correctly to our past which so largely controls our physical behavior and mental attitudes.”
Price then spent two paragraphs making the case that all “forms of life have a similar origin” and that humans and apes “have developed from a common progenitor.” Directly following this, he lamented that “much of modern thinking and teaching have failed to recognize as common the origin of man with many animal forms and its significance for understanding his form and behavior.” The principal importance of this recognition, in Price’s view, was the need to understand that we and all other animal life must obey the same laws of nature in order to thrive.
Price first described how humans differ from “simpler forms of life” by relying not only on instructive instincts, but also willful behavior. This is potentially problematic because our willpower and intelligence are highly variable, so willful behavior opens the opportunity to make mistakes.
He then described in detail the life and reproduction of a tent caterpillar, and concluded that it is all made possible by chemicals “synthesized from the minerals, acids, bases, hormones and vitamins furnished by the rapidly growing green cherry leaves, plus sunshine and atmosphere.” But what if the caterpillar had a will to develop technical savvy, like us?
“Suppose the caterpillar had learned to rob the plant juice of its carotene, then the vitamin A could not form and no eyes could be made or many of the other structures; or if only starches and sugars were eaten, no body could be built or capacity to reproduce and continue the race. Its safety is provided in both its ignorance and the rigidity of Mother Nature’s laws. . . .We humans have the same rigid restrictions regarding food selection as the simpler forms of life when foods are evaluated from their chemical basis. Our greater complicity however, introduces new behavior patterns due to injuries to the structure and therefore the functions of the forebrain. All primitive races that have lived on for long periods have done so by obeying Nature’s rigid laws.”
Price’s ultimate conclusion from this is found in the closing words of the book: “life in all its fullness is this Mother Nature obeyed.”
His point that we and the tent caterpillar must both comply with the laws of nature to thrive is compelling, yet his contention that this somehow depends on recognizing our common ancestry with the tent caterpillar seems at odds with large chunks of his own observations.
For example, on page 322 he discussed how until shortly before the chapter was written, lions, tigers, leopards and other captive felines were not reproducing efficiently. When animal specialists observed African lions taking the organ meats as first choice from slain zebras, human captors began feeding their captive felines organ meats. Lo and behold, they began reproducing. It would seem from this that humans were not consuming poor diets because they considered themselves uniquely exempt among all animal life from the laws of nature. It would rather seem that humans were feeding both themselves and many other animals deficient diets because they did not understand the laws of nature.
Conversely, many if not all of the healthy “primitive” groups Price studied were creationists, and generally supported their obedience to the laws of nature with cultural justifications that had nothing to do with a recognition of common ancestry with animal life. Let us consider these examples:
• The natives of the far north of Canada reported that they derived their dietary wisdom from the teachings of “a great Power.”
• The Tongans did not even acknowledge common ancestry with the white man. When the world was created and populated, they maintained, they were the first to be made, next was the pig, and last the white man.
• The Neur tribe near the Nile in the Sudan ate liver because “they have a belief which to them is their religion, namely, that every man and woman has a soul which resides in the liver and that a man’s character and physical growth depend on how well he feeds that soul by eating the livers of animals.”
• The Swiss consumed the nutrient-rich June butter not because they recognized common ancestry with animals but because they considered it a life-giving gift of God.
It is modern Europeans and Americans who developed a scientific understanding of biological evolution and simultaneously developed a way to make foods that stimulate the pleasure centers in our brains without providing any nutrition. On the other hand, Price himself adhered to this understanding of biological evolution but provided the very foundation for our return to natural, nutrient-dense foods. It thus seems clear from Price’s work that a great diversity of views about human origins can support the willful and humble obedience to nature’s laws that allows the human being to thrive.
WHEAT AND OTHER CEREAL GRAINS
Some writers, mostly in online comment threads and forums, have suggested that the grain-eaters among the groups Price studied fared worse than other groups, or that none of the healthy groups Price studied consumed wheat. As discussed in the sidebar on page 20, making comparisons between groups in this manner is fraught with interpretative problems. Beyond this, however, such statements are simply incorrect.
While tooth decay rates among the oat-eating Gaels (1.2 percent) and the rye-eating Swiss (4 percent) were considerably higher than many other groups consuming their traditional diets (page 441), though still dramatically lower than those consuming modernized diets, Price studied a number of grain-eating African tribes with much lower rates of tooth decay. These include the Chewya at Kisumu, Kenya (page 141), who subsisted on “large quantities of fish . . . together with cereals and sweet potatoes,” and suffered from tooth decay at a rate of only 0.2 percent. Price found the same rate of tooth decay among the Dinkas in Jebelein, Sudan, who similarly subsisted on fish and cereals (page 150).
Among the Bantu (page 150), Price found not a single decayed tooth. Price reported that they lived “largely on dairy products from cattle and goats, together with sweet potatoes, cereals, and bananas.”
It is also important to note that the tooth decay figure for the Swiss (four percent) is likely an inflated estimate of what would occur on the traditional Swiss diet, since Price repeatedly encountered young men and women who reported never having a cavity until they traveled to one or another city around the age of eighteen or twenty, spent a year or two there, and developed rampant tooth decay that came to a halt once they returned home (page 32). Thus, some of the tooth decay Price observed among the Swiss may have resulted from modern diets they consumed while traveling.
Although Price did not directly study any healthy groups that ate wheat as their traditional staple, he did study healthy wheat-eaters. Among about one hundred sixty modernized Native American students at a training school called the Mohawk Institute (page 85), 77 percent had suffered from tooth decay with a total of 17 percent of teeth attacked by cavities. Every single one of these cavities, however, had healed. “The Institute maintained a fine dairy herd,” he wrote, “and provided fresh vegetables, whole wheat bread, and limited the sugar and white flour.” This diet appeared not only to sustain good health, but to reverse damage the students had presumably suffered from more refined diets they had consumed prior to enrolling at the institute.
That whole wheat could make up a substantial proportion of such a healing diet was consistent with Price’s clinical results, where he used rolls made from freshly ground whole wheat as part of his tooth decay reversal program, as well as his animal experiments, wherein he showed that refined wheat but not whole wheat produced cavities in rats.
Although Price didn’t study the Pathans of India himself, he had the following to say about them (page 291): “The most physically perfect people in northern India are probably the Pathans who live on dairy products largely in the form of soured curd, together with wheat and vegetables. The people are very tall and are free of tooth decay.”
Although Price never reported traveling to India, he was familiar with the work of Sir Robert McCarrison (page 479), who studied several groups in that land that thrived on wheat-inclusive diets.
While none of these observations should provide the final word in a debate about the health value of grains, they are important to keep in mind so that when Price’s work is brought up in such a debate, it is presented accurately.
REFERENCES
1. Price, WA. Nutrition and Physical Degeneration: Sixth Edition (16th Printing). La Mesa, CA: Price- Pottenger Nutrition Foundation (2004). All page numbers given in the text refer to this edition.
2. All information on Price’s scientific background is derived from George Meinig’s preface to his own Root Canal Cover Up (Lemon Grove, CA: Price Pottenger Nutrition Foundation, 2004) and Meinig’s introduction, written with S. Hale Shakman, to Price’s Dental Infections, Oral and Systemic (Lemon Grove, CA: Price Pottenger Nutrition Foundation, 2008). Some confusion may be avoided by noting that the American Dental Association had styled itself the National Dental Association from 1897 to 1922, which covers the early period of Price’s tenure.
3. Price WA. Milk Samples Desired for Chemical and Vitamin Determinations. J Heredity. 1929;20(6):302.
4. Mellanby M, Pattison CL. Remarks on the INFLUENCE OF A CEREAL-FREE DIET RICH IN VITAMIN D AND CALCIUM ON DENTAL CARIES IN CHILDREN. Br Med J. 1932;1(3715):507-510.
5. Masterjohn C. Understanding Weston Price on Primitive Wisdom: Ancient Doesn’t Cut It. Wise Traditions. Fall, 2011; 18-23.
6. Wallace, AFC. “Mental Illness, Biology and Culture.” In: Hsu, FLK. Psychological Anthropology. Cambridge, MA: Schenkman Publishing, 1972, pp 363-402.
7. Rejnmark L, Jorgensen ME, Pedersen MB, Hansen JC, Heickendorff L, Lauridsen AL, Mulvad G, Siggaard C, Skjoldborg H, Sorensen TB, Pedersen EB, Mosekilde L. Vitamin D insufficiency in Greenlanders on a westernized fare: ethnic differences in calcitropic hormones between Greenlanders and Danes. Calcif Tissue Int. 2004;74(3):255-63.
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly journal of the Weston A. Price Foundation, Spring 2014.
🖨️ Print post
yes, the Hunzas are the most long-lived people on the planet. They die, some at 180, with a full set of teeth and a full head of hair. They live in a hard to get at place for the western white man (thank goodness). if only the world understood: what you eat is what you are. if you eat good, no doctor is needed. if you eat bad, no doctor can cure….. i eat a similar diet to the hunzas (or what i have read in those london surgeons testimonials who have visited and lived a stint with the hunzas in early twentieth century). i am lucky to live in an isolated (fearfully, growing) area on the west coast of western australia with the antartic winds blowing away any sulphides from the grape spraying and government and farm glyphosate use. i have made myself 80 to 90% self-sufficient. what a shock it was when i recently went to the dentist to find i had many caries and had to have teeth out. what a bigger shock when i found that the dental industry have no products available that are NOT toxic. my ceramic fillings’ glue had rotted and caused decay therein. if you think that sounded bad listen to this: i read a paper on green facts related to dentistry and materials and one section was on the alternatives to amalgam. several of the ceramic fillings were found to be far more toxic and cyto-toxic than their amalgam counterparts. i was shocked when i found out my skin problems, hair loss and memory loss was coming from the aluminium oxide (80%) which made up my ceramic fillings. this material was literally killing me. i didn’t know until my regular hair tissue mineral analysis started coming up with high aluminium readings which got worse as my medical conditions (all around the head area) got worser. the sad thing is australian dentists (even those advertised as bio or natural) just aren’t that. yes, like yuval harari in his book the sapiens stated, the homeo sapiens just doesn’t like the truth. thank you weston price for confirming everything i thought and experienced with my own body and my rescued animals. we all eat a raw, organic, home-grown and home produced diet with filtered (my own charcoal) rainwater. thank goodness for dr igor tabrizian who drew my attention to the study of diagnostic orthomolecular medicine…. thank you sir!
I just read your wonderful comment and would like to thank you for it. I, too, am living in an isolated area in the foothills of the Sierra Nevada mountains somewhat near Yosemite National Park. I raise grass fed, unvaccinated, pasture-raised cattle for beef, organically fed and pasture roaming kunekune pigs for lard and meat, pasture raised, 100% organic supplemented chickens for eggs, and 175 guinea pigs fed 100% organically for their bedding, which is the foundation of my compost. That compost fertilizes my garden and orchard. I’m 80 years old and teach a regenerative, sustainable, organic lifestyle to young people who want to work and learn on a ranch and homestead. One milk goat to make cheese, kefir, yogurt. I, too, suffered aches and pains even though I lived a healthy lifestyle and ate real food. I discovered at 76 years of age that I was not drinking enough water. Someone asked if I’d read the book, “You’re Not Sick, You’re Thirsty” by F. Batmanghedlidj, M.D. I ordered the book and it changed my life. There is a website…www.watercure.com that explains what dehydration does to the body. I drink 2 ounces per one pound of body weight in distilled water in which I put Fulvic Ionic minerals (by Optimally Organic). One must have salt to hold the water in the cells so I lick and eat about 2 tablespoons of Redmonds Real salt (unpolluted) per day after drinking my 6 liters of water (water cannot have salt, lemon juice, apple cider vinegar in it or it becomes “food” and travels a different pathway.) I am an avid reader of Wise Traditions and am grateful for their viewpoints.
Is there any recent scientific evidence or studies that disprove Weston Price’s research for example the root canal is not harmful