






 🖨️ Print post
🖨️ Print post
Translations: Spanish
Exposing Mainstream Myths
by Morton Satin, PhD, Vice President,
Science and Research, The Salt Institute
Aside from water, salt (sodium chloride) is the most ubiquitous food ingredient consumed by humankind. It is a nutrient that is essential to life and good health and has always been the predominant positive ion in extracellular body fluid for all multi-cellular animals.
Having originally evolved from a marine environment, the human body’s salt-to-water ratio is critical to metabolism. Human plasma contains 0.9 percent sodium chloride, most of it coming from food and a small amount from water. The fundamental indicator of salt intake sufficiency points to 1.5 teaspoons (8 grams) of salt per day as the basic human requirement.
SALT IS AN ESSENTIAL NUTRIENT
In clinical studies, salt is calculated in millimoles (mmol) of sodium, where 100 mmol of sodium amounts to 2300 mg which is contained in one teaspoon (5 grams) of salt.
If we do not consume sufficient sodium, our metabolism, driven by specific feedback mechanisms, goes into a sodium-sparing mode so that the circulatory system can maintain osmotic balance and adequate blood pressure. This has several important consequences for us. A reduced intake of sodium is characterized by the stimulation of the renin-angiotensin-aldosterone hormonal system (RAAS). Renin, the first enzyme taking part in the RAAS was clearly shown in a dose-response curve1 to increase as sodium intakes fell below 150 mmol sodium (or 1.5 teaspoons/8 grams of salt) per day. At a point of intake below 110 mmol (6 grams) sodium per day renin begins to rise rapidly. The RAAS feedback mechanism is the most transparent measure of our dose response to salt intake and is a fundamental indicator of sodium intake sufficiency.
Although this cascade of reactions is designed to sustain osmotic balance and blood pressure, chronically elevated levels of renin and aldosterone have significant negative effects on the condition of the circulatory system and may stimulate inflammatory agents within the body. Included among the negative outcomes of chronically elevated levels of renin and aldosterone are insulin resistance,2 metabolic syndrome,3 cardiovascular disease,4 cognition loss,5 and others.
SALT AND BLOOD PRESSURE
The overwhelming public interest in salt consumption derives from the concern over its perceived universal impact on blood pressure (BP). Unfortunately, this has long been a subject of significant myth-information. The cross-population blood pressure response to salt reduction is heterogeneous.6 With major reductions in salt (more than half of our current consumption), about 30 percent of the population will experience a slight drop (2-6 mm) in systolic BP, while about 20 percent will see a similar increase in BP, and the remaining 50 percent of the population will show no effect at all. Considering the relatively small impact of major salt reduction on blood pressure, it is unfortunate that consumers are not aware of all the other negative consequences that occur as a result of dietary salt reduction.
PUBLIC PRESSURE TO REDUCE SALT
In the late 1980s, in response to the notion that sodium had a major impact on a population’s blood pressure, an international study (Intersalt) was carried out to determine the impact of salt consumption on blood pressure.7 As it turned out, the per capita consumption of sodium in the majority of countries ranged between 130-210 mmol sodium or the equivalent of 1.3 to two teaspoons of salt (7-10 grams) per day. The results indicated that there was no clear pattern between the level of salt intake and blood pressure. However, there were four populations among the fifty-two groups that showed very low salt intakes and far lower than average blood pressures. The lowest consumption population in this group was the primitive Yanomami Indians, who live in the Brazilian rain forest. Normally, data points that are very far from the rest of the pattern are referred to as outliers and are generally omitted from the analysis. In this case, the outliers were included and a line drawn from them to the rest of the population in order to show that a pattern relating salt consumption to blood pressure did exist. (See Figure 1.)
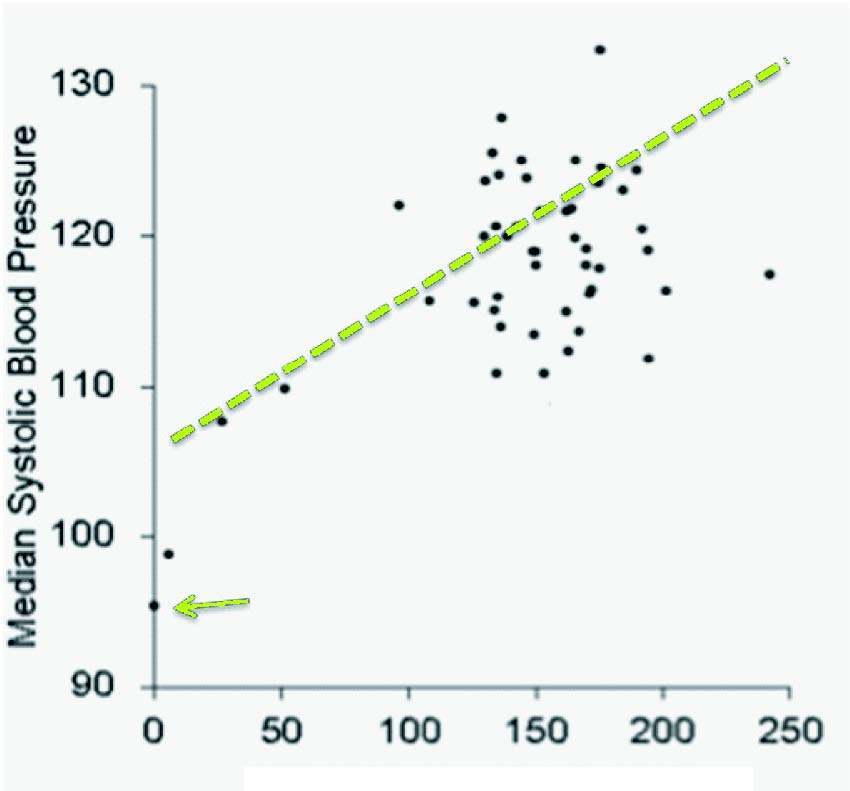
FIGURE 1. InterSalt Study
While the advisability of making comparisons between modern Western societies and those that have vastly different lifestyles, levels of physical activity, caloric intakes and environmental stresses is legitimately open to question, the issue of life-long low BP among the Yanomami was repeatedly used as a justification. The Yanomami are described in the ethnographic literature as an aggressive and violence-prone people. The stress associated with this character along with the continual exposure to environmental stresses does not appear to influence the BP of the Yanomami as they would other population groups. While their abnormal BP profile has been attributed to reduced salt consumption, a far more likely reason appears to be the almost complete absence of a D/D genotype—a genetic trait shared with other Amerindians such as the Xingu Indians of the Amazonian rainforest, one of the other four outlier points. Notwithstanding their lack of an age-related rise in blood pressure, the Yanomami are characterized as a small stature, high mortality and high fertility population with a low life expectancy. It is also interesting to note that despite their long history of evolution in a salt-limited rainforest environment, they have never acclimatized to low sodium intake and have chronically high levels of plasma renin. Nevertheless, the inclusion of the Yanomami data in the formal Intersalt analysis, however misguided, initiated the latest round of salt-restriction efforts.
The supposed merits of significant population-wide dietary salt reductions were further justified through the Rose population strategy theory,8 which contended that most risks to health, including hypertension, were evenly distributed as a continuum across the population rather than being confined to high-risk groups as shown in Figure 2.9
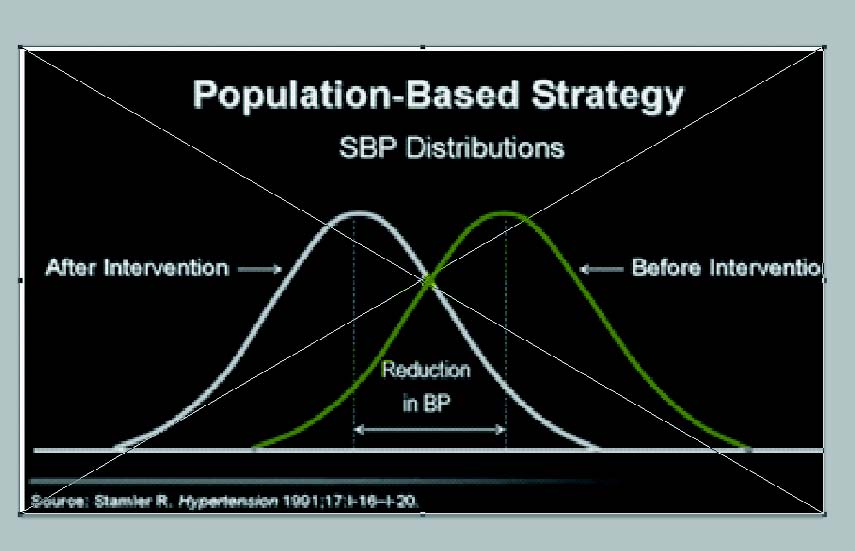
FIGURE 2. Rose Population Strategy
Accordingly, modest risk reductions in BP (such as those achievable through significant salt reduction) across the entire population, including normotensive individuals, might conceivably reduce the population incidence of cardiovascular disease. This inspired the idea that a great number of lives and millions of dollars in health care costs might be saved through dietary salt reduction. But this notion appears to have a number of obvious flaws.
In the first instance, salt sensitivity and the tendency towards elevated blood pressure is largely driven by genetics and thus not evenly distributed, but rather highly skewed across the population. In addition, if an intervention such as dietary salt reduction demonstrated even a small negative effect (such as any one of the outcomes resulting from stimulation of the renin-angiotensin- aldosterone system), this would tend to shift the risk curve in the opposite direction and result in greater risk of morbidity and mortality. Finally, any intervention that might statistically benefit the public health (such as an insignificant drop in BP) may not translate into any difference at all to an individual’s health—commonly referred to as the “Population Paradox.”10 Considering the apparent shortcomings to this theory, it is remarkable that it was so widely and uncritically accepted.
FLAWED STANDARDS
The intellectual stage was thus set to establish standards on salt consumption that were fundamentally flawed. And that’s exactly what happened with the Dietary Reference Intakes (DRI) for sodium. In fact, they sank a great deal further into the mire of medical myth-information. The DRI for sodium, the foundation publication for our current recommendations for salt consumption, clearly state at the outset that “Because of insufficient data from dose-response trials, an Estimated Average Requirement (EAR) could not be established, and thus a Recommended Dietary Allowance could not be derived. Hence, an Adequate Intake (AI) is provided.”11
This single statement concedes, from the very beginning, the shift away from an evidence-based approach in establishing recommendations to one of subjective inference: opinion. Rather than a plea for more research to enhance the insufficient base of evidence, the text presents a blunt fiat, based upon expediency rather than anything else. The AI was arbitrarily set by the DRI committee at 1,500 mg sodium or a little more than one half teaspoon (3 grams) of salt per day for young adults “…to ensure that the overall diet provides an adequate intake of other important nutrients and to cover sodium sweat losses in unacclimatized individuals who are exposed to high temperatures or who become physically active…” However, no supporting information on young adults was provided to confirm that this arbitrary figure was in any way justified. In fact, this opinion has since been shown to be incorrect.12
The case for setting the upper limit of salt consumption at the equivalent of 100 mmol (2,300 mg) sodium or one teaspoon (8 grams) of salt per day appeared even more problematic. Rather than determining the body’s integrated response to various levels of salt; i.e., the normal and rational dose response methodology used for all nutrients, it was clear from the start that the overwhelming preoccupation with just one surrogate measure for cardiovascular disease—blood pressure—would remain the singular focus: “The major adverse effect of increased sodium chloride intake is elevated blood pressure, which has been shown to be an etiologically related risk factor for cardiovascular and renal diseases.” Furthermore, the use of precisely 100 mmol sodium (contained in 5 grams or one teaspoon of salt) was not the result of any dose-response relationship involving an established suite of health outcomes. It was nothing more than an arbitrary and convenient set point from which to observe any reductions in blood pressure (regardless of how small) when sodium intakes were decreased.
Nevertheless, this was the intellectually bankrupt basis upon which the recommendations for salt were set, with full confidence that the public acceptance of salt-health mythology would serve to allay any critical scrutiny. What were these salt myths?
MYTH 1:
We eat more salt today than ever before.
FACT: Our current salt consumption (1.5 to 1.75 teaspoons per day, 8-9 grams) is about one half of the amount consumed between the War of 181213 and the end of World War II,14 which was about three to 3.3 teaspoons (16-17 grams) of salt per day.
MYTH 2:
Our knowledge of the major sources of salt in our diet (i.e., 80 percent from processed foods) is unquestionable.
FACT: These data, referred to in every medical publication, is based on a single paper from 1991, which involved a dietary recall (a very unreliable method of data gathering) of a total of just sixty-two persons.15
MYTH 3:
Our salt consumption continues to rise every year.
FACT: There has been no change in our consumption of salt since the mid-1950s.16
MYTH 4:
The thirty-year public health initiative in Finland represents a successful model of salt reduction.
FACT: While Finland was able to reduce salt consumption among its population from 2.3 teaspoons of salt (12 grams) per day down to 1.3 teaspoons (7 grams) per day in the period from 1970 to 2000 (in much the same way that the U.S. did from 1945-1960), the health benefits that they have achieved during the same time period were no better (and, in fact, marginally worse) than neighboring and other countries that did not reduce salt consumption.
MYTH 5:
Current levels of salt consumption result in premature cardiovascular disease and death.
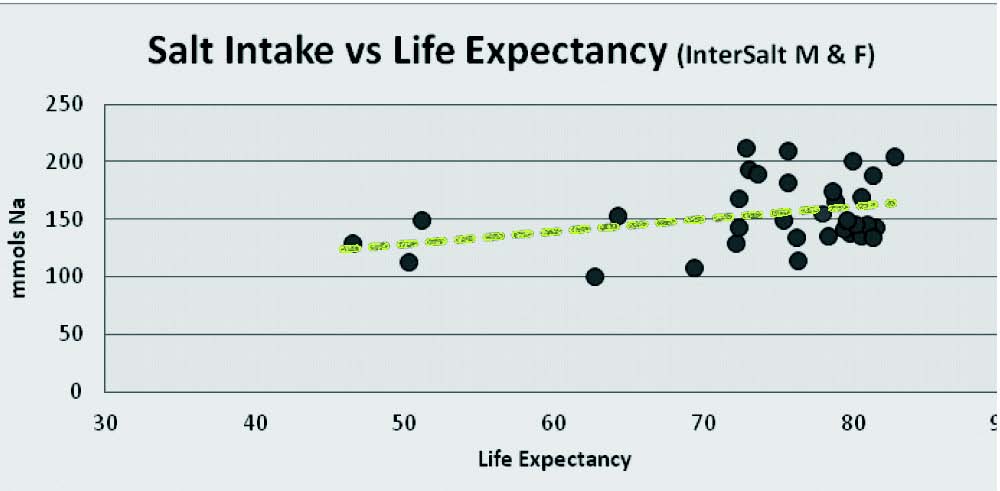
FACT: When average life expectancy in various countries is plotted against the average salt intake in those countries, it is clear that the higher the salt consumption, the longer the life expectancy. (See Figure 3.) While no cause-and-effect relationship between sodium intake and lifespan is implied, the data clearly demonstrate the compatibility between life expectancy and the associated levels of sodium intake.
FIGURE 3. InterSalt Life Expectancy
MYTH 6:
Cutting back on salt will improve the overall diet.
FACT: Salt makes the bitter phytochemicals in salad greens and vegetables more palatable. Removing salt from dressings or accompaniments will make these important diet items less acceptable and will discourage people from eating them.
MYTH 7:
Reduced salt levels are critical to the DASH diet.
FACT: When the results of the DASH Sodium trial are examined (see diagram in Figure 4), it is immediately apparent that merely moving to a DASH diet (red line) has a significantly greater impact on blood pressure than simply lowering salt consumption. Dropping from the normal level of sodium consumption to the Dietary Guidelines’ recommended level reduced the systolic pressure in the American diet (blue line) by an average of 2.1 mm Hg. However, simply changing from a
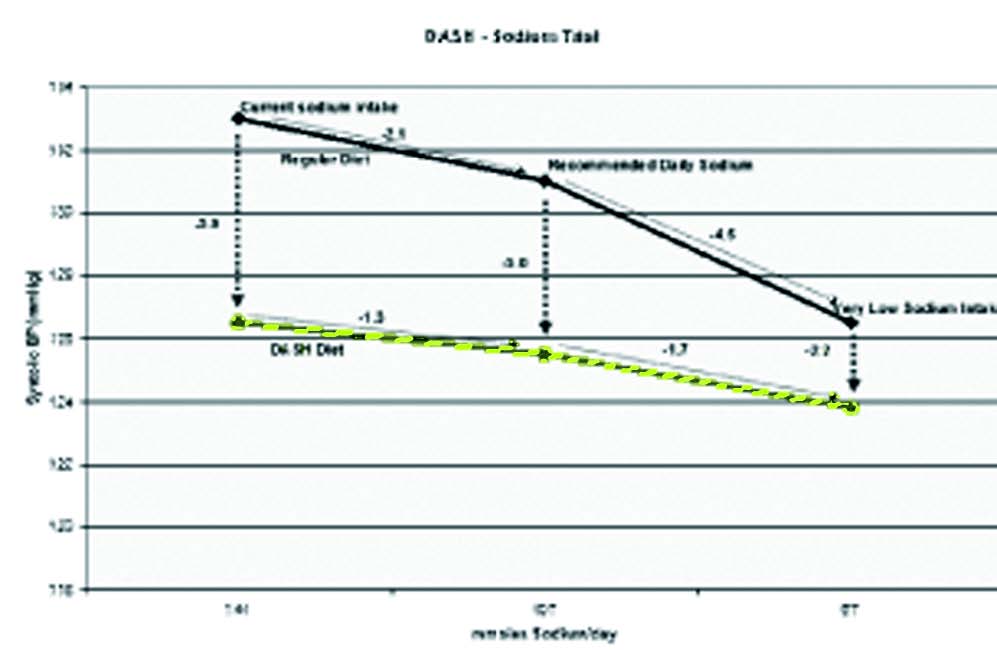
standard American diet to the DASH diet, without any changes to sodium consumption, reduced the systolic blood pressure by 5.9 mm Hg, almost three times the drop resulting from the recommended sodium reduction. More important, reducing salt makes the DASH diet far less palatable and thus discourages people from adopting it.
FIGURE 4. The DASH Sodium Trial
MYTH 8:
There is a clear relationship between salt intake and blood pressure.
FACT: The lack of a clear relationship between salt intake and blood pressure is best exemplified with the standard hospital saline IV drip, which supplies an average of three liters of 0.9 percent sodium chloride per day. This is equivalent to twenty-seven grams of salt (4.5 teaspoons) per day while in the hospital in addition to the six grams (one teaspoon) of salt taken in food (if the Guidelines are followed). That is a total of thirty-three grams of salt per day or more than five times the Dietary Guideline recommendations! Yet patients’ BP is checked every four to six hours and does not change. Where is the purported relationship of salt intake to blood pressure?
MYTH 9:
Reducing salt intake can do no harm.
FACT: Reduced salt intakes have repeatedly been linked in the medical literature to the following conditions:
• Insulin resistance (diabetes)
• Metabolic syndrome
• Increased cardiovascular mortality and readmissions
• Cognition loss in neonates and older adults
• Unsteadiness, falls, fractures
• Lifelong avidity for salt
• And more
MYTH 10:
The U.S. Dietary Guidelines process is valid.
FACT: The original Dietary Recommended Intakes (DRI), issued under the imprimatur of the Institute of Medicine (IOM) (National Academy of Sciences), were immediately accepted internationally and spared the critical scientific review normally given to nutritional recommendations. Indeed, any conscientious perusal of the document reveals the numerous compromises and rationalizations made in lieu of actual evidence in order to arrive at the final recommendations. This was reiterated during a 2007 IOM workshop entitled, “The Development of DRIs 1994–2004: Lessons Learned and New Challenges,”17 where several participants stressed that the DRIs were largely based on the lowest quality of information—opinion—rather than on randomized controlled clinical trials which represent the highest quality of evidence. Yet the disposition of the DRIs provides an insight into how far we have strayed from the scientific principle of adherence objectivity and evidence-based medicine.
The five-year Dietary Guidelines for Americans (DGA) review process has always been publicized as being an “independent and objective” reevaluation of the previous DGAs. The 2005 DGA for sodium referred to the DRIs as a foundation document and assumed all its recommendations. The consequent 2010 DGAs reconfirmed the recommendations of the 2005 DGAs with the proviso that the at-risk populations consume 1,500 mg sodium (1/2 teaspoon/3 grams salt) per day for the upper limit. As it happened, the Chair of the original DRIs committee that set the first recommendations for sodium also happened to serve as the Chair of the 2005 Dietary Guidelines Subcommittee on Electrolytes and thus evaluated the very recommendations that he was responsible for promulgating in the first place.
In 2010, the process was repeated and, once again, the same Chair of the Subcommittee on Electrolytes ran the show. This sequence, fully sanctioned by the Institute of Medicine and the U.S. Department of Agriculture, begs the question as to whether any “independent and objective” analytical process can feature a single individual piloting the creation of standards (DRIs) who then is charged with evaluating his own recommendations five years later, and asked once again to evaluate his prior evaluations. This process makes a sham of the concept of independent, objective evaluations and makes a mockery of the integrity of our great scientific institutions!
WHERE ARE WE NOW?
Notwithstanding the myths and limitations described above, the recommendations for sodium have been accepted, without reservation, by virtually every public health agency around the world. Yet, despite the near impossibility of goal achievement in practical terms, the recommendations appear to represent a level of consumption that results in no more than mid-single digit reductions in systolic BP for a limited portion of the population and a similar sized increase in BP for another limited portion of the population. Several meta-analyses have seriously questioned the purported long-term benefits of population-wide salt reduction,18-21 while others have vigorously supported it.22
In fact, conflicting comment and repeated parsing of the “evidence” has become a regular feature of the salt-and-health debate, leading some journalists to complain that “almost every nutritional ‘fact’ is in reality an opinion, often based on poor quality evidence.”23 Considering that overall good health comprises considerably more than a single digit blood pressure response, the current dietary recommendations have served as a decades-long red herring obscuring the need for more research to get more and better dose-response data.
A BETTER UNDERSTANDING OF SALT NEEDS
Several recent publications appear to get us closer to what may be considered to be the human requirement for salt. For example, a very recent study from Harvard Medical School demonstrated that when healthy people were placed on a very low-salt diet (20 mmol sodium or a fifth of a teaspoon (1 gram) of salt per day), they developed insulin resistance within seven days.24 Those placed on high salt diets (150 mmols or 1.5 teaspoons/8 grams of salt) showed no such effect. We conclude that low-salt intakes warrant further investigation in the pathogenesis of diabetes and cardiovascular disease.
In a series of three analyses of consecutive National Health and Nutrition Examination Surveys (NHANES I,25 II ,26 and III27 ), researchers were unable to demonstrate any survival advantage resulting from low-sodium diets; on the contrary, a modest relationship between increased all-cause mortality and low-sodium diets was observed (although non-significant).
A recent study conducted to examine the health outcomes related to salt intake (as measured by twenty-four-hour urinary sodium), demonstrated that lower sodium excretion was associated with an increased risk of cardiovascular death, while higher sodium excretion did not correspond with increased risk of hypertension or cardiovascular disease complications.28 Another meta-analysis of one hundred sixty-seven studies by Graudal and co-workers29 confirmed and expanded upon previous reports that significant dietary sodium restriction from greater than or equal to 150 mmol sodium (1.5 teaspoons/8 grams of salt) per day down to a level of less than or equal to 120 mmol sodium (1.2 teaspoons/6 grams of salt) per day resulted in limited but significant reductions in blood pressure. In white subjects who were hypertensive, the mean reduction was 5.5 mm Hg systolic and 2.8 mm Hg diastolic. For white normotensive subjects these figures dropped down to 1.3 mm Hg systolic and 0.1 mm Hg diastolic. However, the meta-analysis went further to confirm and quantified the unfavorable impacts that sodium restriction had on several other risk factors for cardiovascular disease. These included significant increases in renin, aldosterone, catecholamines (adrenaline, noradrenalin) and lipids (cholesterol and triglycerides). Renin and aldosterone were of particular concern as they have been repeatedly associated with increases in cardiovascular mortality in long-term follow-up studies.
During his Presidential address to the International Society of Hypertension, Alderman referred to a J-shaped response to describe the broader impact of sodium intake on health outcomes, referring to evidence of harm observed at the low and high extremes of consumption, with the least impact noted in a broad middle range centered around 3,500 mg sodium or 1.5 teaspoons/8 grams of salt per day.30
In a recent study, published in the Journal of the American Medical Association (JAMA),31 researchers found moderate salt intake to be associated with the lowest risk of cardiovascular events, whereas low intakes, equivalent to less than or equal to 3,000 mg sodium or 1.5 teaspoons (8 grams) of salt per day, were associated with an increased risk of cardiovascular death and hospitalization for congestive heart failure, and higher intakes of more than 7,000 mg sodium or three teaspoons (15 grams) of salt per day, were associated with an increased risk of stroke, heart attack and other cardiovascular events. Once again, a J-shaped curve appeared to describe the dose-response relationship.
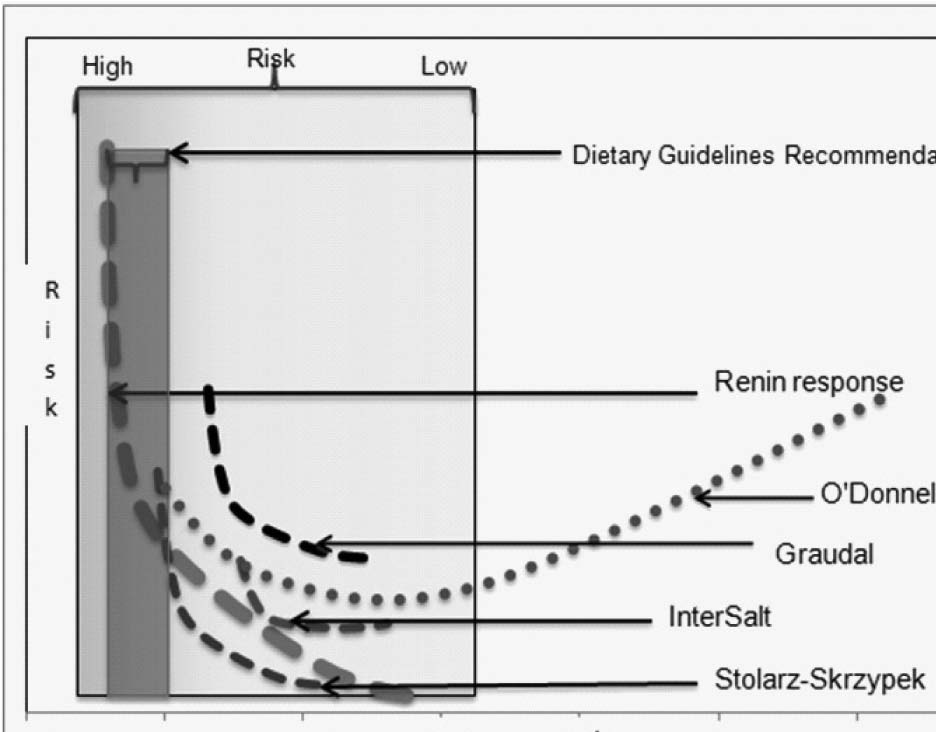
FIGURE 5. Consolidated Study Results
The J-shaped or U-shaped curve is a common dose-response occurrence for essential nutrients in both plant and animal species.32 French nutritionist, Gabriel Bertrand, mathematically described the original relationship in 1912.33 What is now known as Bertrand’s Rule applies to a great many micro- and macronutrients. At very low levels of intake, where there is insufficient nutrient flux to support the full range of associated physiological functions, there is a high risk of adverse effects. This is considered the deficiency range. If the adverse effects don’t result in acute catastrophic events, individuals may survive, although at a diminished potential. As the level of nutrient is increased to a point where the deficiency disappears, minimal adverse effects are experienced and homeostasis is established. Continually increasing intake leads to exceeding the homeostasis requirement and adverse effects reappear (though not necessarily the same ones).
Although there is a quantity of data describing storage of sodium within the body, it is difficult at this stage to speculate what role storage plays in maintaining physiological homeostasis. It therefore remains for us to determine what type of data are available to give us an indication of the optimum level of consumption. Simply from a biological feedback perspective, the point at which a deficiency of salt elicits an increase in renin production must be considered a basic biological indicator. Using the study of Alderman, et al.,1 anything less than 170 mmol (3,910 mg) sodium per day (1.7 teaspoons/9 grams salt) appears as a starting point. As increases in renin only occur when sodium intake is insufficient, these data do not permit an estimate for an upper limit.
SALT CONSUMPTION AND LIFE EXPECTANCY
Average life expectancy is often considered a measure of the overall health of a population, (although infant mortality in some countries can be a confounding factor). Comparing the InterSalt study data on average sodium consumption in thirty-two countries around the world34 with life expectancy results in the following picture. If we take the top 20 percent with greatest life expectancy, their sodium intake ranges from 140–205 mmol per day, averaging around 170 mmol (1.75 teaspoons of salt/9 grams). While no cause-and-effect relationship between sodium intake and lifespan is implied, the data do demonstrate the compatibility between life expectancy and the associated levels of sodium intake.
While not providing a continual dose-response relationship, the data in the recent Graudal paper29 illustrate a series of responses to reducing salt consumption from more than 150 mmol (1.5 teaspoons/8 grams of salt) down to less than 120 mmol sodium (1.2 teaspoons/6 grams) per day. Together with a small but significant reduction in blood pressure, there is also a concomitant significant increase in several other risk factors for diabetes and cardiovascular disease. Again, while no continual dose response relationship is implied, the risks appear to outweigh the benefits when reducing sodium consumption below 3,450 mg (1.5 teaspoons/8 grams) per day.
Consistent with the NHANES studies,25-27 the paper demonstrated significant increases in cardiovascular mortality as consumption of sodium dropped from a high of 260 mmols (just over 2.5 teaspoons/13 grams of salt) down to a low of 107 mmols (a bit more than one teaspoon).
Finally, based on a long-term study with a large cohort, the O’Donnell paper31 sets out a J-shaped response curve with the range of lowest risk between a daily consumption of 1.3 (7 grams) and three teaspoons (15 grams) of salt per day.
If the data from the above studies are compiled, it is apparent that the range of sodium intake at which there is least negative health outcome impact is anywhere above approximately 3,000 mg per day or the equivalent of 1.3 teaspoons (7 grams) of salt. This also happens to be the range that most people around the world consume. These data are not based on surrogate end points, but on hard outcomes (mortality) and dose responses involving measurable feedback responses (renin, aldosterone, catecholamines, cholesterol and triglycerides) that, in the words of the DRIs, are not subject to “imprecision in blood pressure measurement.”
These results support the idea that sodium is consumed in a fairly narrow hygienic range,35 which has more recently been approximated as 2,691-4,876 mg sodium or between 1.2 (6 grams) and 2.13 teaspoons (11 grams) of salt per day.36
Considering the available evidence, it is difficult to determine a practical maximum for salt because the data suggest that such a level is outside our current consumption range; i.e., greater than 7,000 mg sodium or the equivalent of three teaspoons (15 grams) of salt per day. In other words, our taste response to salt may be self-limiting.
HISTORICAL RATES OF SALT CONSUMPTION
It is of great interest that available data suggest Western societies consumed between three and 3.3 teaspoons (15-17 grams) of salt per day from the early 1800s until the end of World War II, based on military archives for prisoner-of-war and soldier rations around the world. During the Anglo-American War of 1812, despite its high cost, salt rations amounted to three teaspoons (15 grams) per day.37 American prisoners of war, incarcerated in Britain’s Dartmoor prison, bitterly complained that the 1.5 teaspoons (8 grams) of salt per day they received was part of “…scanty and meager diet for men brought up in the land of liberty, and ever used to feast on the luscious fruits of plenty…”38 Declassified World War II documents regarding rations fed to American prisoners of war show a ration of one hundred forty grams per week or 3.3 teaspoons (17 grams) per day.39
After World War II, when refrigeration began to displace salt as the main means of food preservation, salt consumption in the U.S. (and somewhat later in other countries) dropped dramatically to about half that rate, or nine grams (1.8 teaspoons) per day and, based on twenty-four hour urinary sodium data, has remained flat for the last fifty years.40 During that time, rates of hypertension have increased,41 thus casting doubt on any linkage between the two.
It is telling that this sudden drop took place without pressure or influence from any government Dietary Guidelines, public health institutions or strident warnings from salt-reduction advocates. The massive reduction was the result of an effortless shift to a palatable, cold-chain-based food supply. It is further interesting that this abrupt drop halted at one level of consumption fifty years ago and descended no further. It is equally extraordinary that, without guidance or pressure of any kind, the consumption of salt around the world, for more than two centuries has remained in the range of 1.5 to three teaspoons (8-15 grams) per day, which, from all the available data, appears to hold the lowest risk for us. It lends support to the notion of the “wisdom of the body” at work through a mechanism that may not be as obvious as the typical sodium appetite so common in most other mammalian species, but effective nevertheless.
Regardless of the evidence, we now must face a certain reality resulting from the two decades-long campaign to reduce salt. Because the Dietary Reference Intakes for salt were promulgated by the Institute of Medicine, they were immediately adopted without question by most public health agencies around the world. This position, repeated and amplified by an uncritical press influenced the food industry to consider salt reduction strategies very seriously, not because there was genuine concern for the impact of salt on health, but for two commercial considerations. The first was the concern related to public pressure as the food industry did not want to be perceived as purveyors of unhealthy products. Second, reduced salt product formulations had the potential to become new “low salt” varieties that might capture additional market share.
Salt reduction initiatives are now the largest product development expenditure in the processed food industry, and the chemical senses research institutes—which played a critical role in promoting salt reduction strategies42—are the major recipients of these research funds. Advancements in chemistry may result in reduced-sodium products that have acceptable taste profiles for consumers. If this does occur, the question remains how a reduced-salt food supply might impact the health of the public.
Early indications from the UK indicate that while the salt content of processed foods is reduced, the sales of table salt appear to have increased dramatically.43 Unfortunately, this phenomenon is complicated by the habit of using table salt for de-icing home steps and sidewalks in the UK. As yet, no solid relationship has been established between reduced salt in processed food formulations and increased use of table salt. The results of the Food Standards Agency (FSA) UK salt survey are due in 2012 and it may be possible to determine whether urinary sodium levels have indeed fallen. The 2011 FSA salt survey results coming out of Scotland44 indicate that this had not occurred as yet, and consumers do appear to be making up for the significantly reduced salt levels in processed foods through some means.
If this is indeed the case, a question to consider is whether our relatively stable consumption of salt around the world is the result of our avidity for the taste of salt or a physiological sodium appetite mechanism that drives us to seek out a particular level of salt. This is a critical question. If advances in salt reduction chemistry are able to trick our taste senses and there are no other physiological mechanisms at work, then consumers will be able to reduce their salt consumption, perhaps even as far down as to the DGA recommended levels of 1,500–2,300 mg sodium (a little more than one-half to one teaspoon/3-5 grams of salt) per day. If that were to be the case, then the reported population-wide risks associated with increased plasma renin and aldosterone, catecholamines, cholesterol and triglycerides would be of concern and people may die prematurely as a result.
If, on the other hand, there is some form of sodium appetite mechanism at work, then the chemistry directed at deceiving our taste senses should not be particularly effective, since our hunger for salt would result from something other than organoleptic pleasure. If this were the case, then there is a possibility that reducing salt in processed foods may stimulate increased consumption of food, simply to achieve a set level of sodium intake, thereby exacerbating the obesity epidemic. (The sodium appetite mechanism is currently applied commercially to cattle finishing feed, where total intake is controlled by adjusting the level of salt content. Reducing the salt content stimulates cattle to consume more feed, while increasing salt has the opposite effect.)
Aside from the previous risks noted, there is a possibility that reduced salt in processed food formulations will affect dietary choices. The nutritious phytonutrients associated with dark green vegetables and salads are bitter and generally more palatable with salt added directly, through dressings or in processed accompaniments. The heart-healthy diet practiced around the Mediterranean Basin is considerably higher in salt than that in most Western European and North American countries, because so many of the traditional foods they consume are still preserved with salt. However, salads and vegetables make up a large part of that diet and salt is used liberally to ensure palatability. (The Latin derivation of the word “salad” is “sal,” and refers to salted vegetables.) A reduced dietary salt intake may discourage consumption of salads and vegetables, particularly among children.45 In the UK, where salt has been removed from many school lunches, students avoid their vegetables until they get home. Writing in the UK Telegraph, journalist Paul Eastham complained that since the school ban on salt shakers, his daughter stopped eating vegetables, because they are so bland.
“All the goodness they promise to deliver remains untouched on the plate—a complete waste of nutrients, health potential and money—all because they remain unpalatable…. My daughter might not touch the ‘bland’ vegetables at school, but at home—where she is allowed to use salt—she clears her plate.”46
We appear to be at a crossroads in the salt-health debate. The decades-long impasse regarding the merits of population-wide salt reduction can only be resolved with conclusive research—not to delay the implementation of public health policies but to substantiate them before they are imposed on the public. The study that would best serve the needs of consumers and public health agencies alike would be a large-scale, long-term, randomized, controlled trial on the impact of reduced salt intakes on a suite of agreed health outcomes—not surrogate measures. Considering the food industry’s current focus and expenditures on salt reduction efforts, it is in its interest to financially support such a trial, if only to confirm the importance of their ongoing salt reduction efforts.
REFERENCES
1. Alderman MH, Madhavan S, Ooi WL, Cohen H, Sealey JE, Laragh JH. Association of the renin-sodium profile with the risk of myocardial infarction in patients with hypertension. N Engl J Med. 1991;324:1098–1104.
2. Garg R, Williams GH, Hurwitz S, Brown NJ, Hopkins PN, Adler GK. Low-salt diet increases insulin resistance in healthy subjects. Metabolism – Clinical and Experimental. 2011;60(7):965-968.
3. Nakandakare E, Charf A, Santos F, et al. Dietary salt restriction increases plasma lipoprotein and inflammatory marker concentrations in hypertensive patients. Atherosclerosis. 2008;200:410–6.
4. Stolarz-Skrzypek K, Kuznwtsova T, Thijs L, et al. Fatal and nonfatal outcomes, incidence of hypertension, and BP changes in relation to urinary sodium excretion. JAMA. 2011;305:1777-1785.
5. Renneboog B, Musch W, Vandemergel X, Manto MU, Decaux G. Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am J Med. 2006;119(1):71.e1-8.
6. Miller JZ, Weinberger MH, Daugherty SA, Fineberg, NS, Christian JC, Grim CE. Heterogeneity of blood pressure response to dietary sodium restriction in normotensive adults. J Chron Dis. 1987:40(3):245-250.
7. Intersalt Cooperative Research Group. Intersalt: an international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. BMJ. 1988;297(6644):319-328.
8. Rose G. Sick Individuals and Sick Populations. International Journal of Epidemiology. 1985;14(1):32-38.
9. Stamler R. Implications of the INTERSALT study. Hypertension. 1991;17(Suppl 1):I16–I20.
10. Chariton BG. A critique of Geoffrey Rose’s “population strategy” for preventive medicine. J R Soc Med. 1996;88:607-610.
11. National Research Council. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate.: The National Academies Press, Washington, DC. 2005:p. 270.
12. Maillot M, Drewnowski A. A Conflict between Nutritionally Adequate Diets and Meeting the 2010 Dietary Guidelines for Sodium. Am J Prev Med. 2012;42(2):174-179.
13. Rations: The History of Rations, Conference Notes, Prepared by The Quartermaster School for the Quartermaster General, January 1949, accessed at http://www.qmfound.com/history_of_rations.htm on 12/20/2011.
14. American Prisoners Of War In Germany, Prepared by Military Intelligence Service War Department, November 1945, Restricted Classification Removed-STALAG 17B (Air Force Non-Commissioned Officers) accessed at http://www.valerosos.com/AMERICANPRISONERSOFWAR.pdf on 12/20/2011.
15. Mattes RD, Donnelly D. Relative contributions of dietary sodium source. J Am Coll Nut. 1991;10(4):383-93.
16. Bernstein AM, Willett WC. Trends in 24-h urinary sodium excretion in the United States, 1957-2003: a systematic review. Am J Clin Nutr. 2010 Nov;92(5):1172-80. Epub 2010 Sep 8.
17. Food and Nutrition Board, Institute of Medicine, “The Development of DRIs 1994-2004: Lessons Learned and New Challenges. Workshop Summary,” accessed at: http://www.iom.edu/Reports/2007/The-Development-of-DRIs-1994-2004-Lessons-Learned-and-New-Challenges-Workshop-Summary.aspx on 1/12/2012.
18. Hooper L, Bartlett C, Davey SG, et al. Advice to reduce dietary salt for prevention of cardiovascular disease. Cochrane Database Syst Rev. 2004;(1):CD003656.
19. Jurgens G, Graudal NA. Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterols, and triglycerides. Cochrane Database Syst Rev 2004; (1):CD004022.
20. Assessment of Non-drug Treatment Strategies in Patients with Essential Hypertension: Reduction in Salt Intake (Nutzenbewertung Nichtmedikament? Ser Behandlungsstrategien Bei Patienten Mit Essenzieller Hypertonie: Kochsalzreduktion). Institute for Quality and Efficiency in Health Care. Executive Summary of Report A05-21B, 2009. Benefit Cologne, Germany: Executive Summary of Meta-analysis in English.
21. Taylor RS, Ashton KE, Moxham T, Hooper L, Ebrahim S. Reduced Dietary Salt for the Prevention of Cardiovascular Disease: A Meta-Analysis of Randomized Controlled Trials [Cochrane Review]. Am J Hyperten. 2011;24(8):843–853.
22. He FJ, MacGregor GA. Effect of longer-term modest salt reduction on blood pressure. Cochrane Database of Systematic Reviews. 2004, Issue 3. Art. No.: CD004937.
23. Hawkes N. Take dietary truths with a pinch of salt. BMJ. 2011;343:d5346.
24. Garg R., Williams GH, Hurwitz S, Brown NJ, Hopkins PN, Adler GK. Low-Salt Diet Increases Insulin Resistance in Healthy Subjects, Metabolism. 2010;60(7):965-68. Epub 2010 Oct 30.
25. Alderman MH, Cohen H, Madhavan S. Dietary sodium intake and mortality: the National Health and Nutrition Examination Survey (NHANES I). Lancet. 1998;351(9105):781-5
26. Cohen HW, Hailpern SM, Fang J, Alderman MH, Sodium intake and mortality in the NHANES II follow-up study. Am J Med. 2006;119(3):275.e7-14.
27. Cohen HW, Hailpern SM, Alderman MH, Sodium intake and mortality follow-up in the Third National Health and Nutrition Examination Survey (NHANES III). J Gen Intern Med. 2008;23(9):1297-302. Epub 2008 May 9.
28. Ibid.
29. Graudal NA, Hubeck-Graudal T, Jürgens G. Effects of low-sodium diet vs. high-sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride (Cochrane Review). Am J Hypertens 2011;25:1–15.
30. Alderman M. Dietary Sodium and cardiovascular disease: the ‘J’-shaped relation. J Hypertens. 2007:25;903-907.
31. O’Donnell MJ, Yusuf S, Mente A, Gao P, Mann JF, Teo K, McQueen M, Sleight P, Sharma AM, Dans A, Probstfield J, Schmieder RE. Urinary sodium and potassium excretion and risk of cardiovascular events. JAMA. 2011 Nov 23; 306(20):2229-38.
32. Mertz W, The essential trace elements. Science. 1981:213:580–583.
33. Bertrand G. On the role of trace substances in agriculture. Eighth Int. Congr, Appl. Chem. 1912;28:30-40 .
34. INTERSALT Cooperative Research Group: INTERSALT:An international study of electrolyte excretion and blood pressure. Results for 24-hour urinary sodium and potassium excretion. Br Med J. 1988;297:319-330.
35. Folkow B. Salt and Hypertension. News in Physiological Sci. 1990;5;220-224.
36. McCarron DA, Geerling JC, Kazaks AG, Stern JS. Can Dietary sodium intake be modified by public policy? Clin J Am Soc Nephrol. 2009;4:1878-1882.
37. Rations: The History of Rations, Conference Notes, Prepared by The Quartermaster School for the Quartermaster General, January 1949, accessed at http://www.qmfound.com/history_of_rations.htm on 12/20/2011.
38. James Adams, Dartmoor Prison, A Faithful Narrative of the Massacre of American Seamen, to Which is added a Sketch of the Treatment of Prisoners During the Late War by the British Government (Pittsburgh, S. Engles, 1816), accessed at http://www.archive.org/stream/prisonersmem00andr#page/12/mode/2up/search/salt on 12/20/2011.
39. American Prisoners of War in Germany, Prepared by Military Intelligence Service War Department, November 1945, Restricted Classification Removed – STALAG 17B (Air Force Non-Commissioned Officers) accessed at http://www.valerosos.com/AMERICANPRISONERSOFWAR.pdf on 12/20/2011.
40. Bernstein AM, Willett WC. Trends in 24-h urinary sodium excretion in the United States, 1957-2003: a systematic review. Am J Clin Nutr. 2010;92(5):1172-1180. Epub 2010 Sep 8.
41. Ayala C, Croft JB, Wattigney WA, Mensah GA. Trends in Hypertension-Related Death in the United States: 1980- 1998. J Clin Hypertens. 2004;6(12):675-681.
42. Institute of Medicine. Strategies to reduce sodium intake in the United States. Washington, DC: National Academies Press; 2010.
43. Watson E. FSA: Salt sales might be up, but consumption is down. Food Manufacture.CO.UK. 18 June 2010. Accessed at http://www.foodmanufacture.co.uk/Sectors/Healthyfoods/FSA-Salt-sales-might-be-up-but-consumption-is-down on 1/11/2012.
44. Scottish Centre for Social Research. A survey of 24 hour urinary sodium excretion in a representative sample of the Scottish population as a measure of salt intake. April 2011. Accessed at http://www.foodbase.org.uk//admintools/reportdocuments/681-1-1229_S14047.pdf on 1/11/2012.
45. Balitsis JK. Impact Of Sodium Chloride On Liking Of Cruciferous Vegetables. 2008, Master of Science Thesis, Ohio State University, Columbus, OH.
46. Paul Eastham, “Take this ban with a pinch of salt,” London Telegraph, Nov., 13 2006, accessed at http://www.telegraph.co.uk/health/main.jhtml?view=DETAILS&grid=&xml=/health/2006/11/13/hsalt13.xml, on Dec.6, 2007.
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly journal of the Weston A. Price Foundation, Spring 2012.
I noticed that no reference was made regarding whether table salt or sea salt was used in these studies. I imagine that studies of sodium intake (for sodium/salt added to foods) refer to table salt. I wonder how different the results would be if the same studies would be done with sea salt and if tests to measure increase/decrease in blood pressure and other health issues would yield different results.
Hi Caryn,
you ask : Caryn: Thank you for bringing up a valid issue. I would love to know the difference in health benefits between sodium cloride and sea/mineral salts on the human body, especialy their effects on blood bressure as I have had several clients in the past with that question and issue. Does anyone down the line have info or opinion on the subject? you can read my update of the article I have complied about salt and also unrefined salts advantages over refined salt go to the further reading tab at the top of the page http://www.regenerativenutriti…t-p-74.asp
This link is dead. I would love a science based comparison of different salt on the market, as well as details of refinement processes and additives.
salt amount daily
I think the advice about how much salt daily (as well as to use as much as possible unrefined sea salt, preferably Celtic salt) to use should be clarified thus:
A very slightly rounded teaspoon (it may appear as level to most poeple you actually have to shake some off to really get a level teaspoon) actually contains 4 grams. This is consitant with the fact that the desity of salt is is higher than 1. Fairly fine grain celtic salt comes in at a density of 1.1 , but finer salts would be more dense.
It should also be stated that the teaspoon we are refering to is a common (small) domestic teaspoon that can hold 3 ml of water whereas the larger medicinal teaspoon can hold 5 mls water.
In summary then I suggest the daily amount recommeded if we are talking about teaspoons should state: Suggested use from a slightly rounded (common 3 ml) teaspoon (approx 4 g) to 2 slightly rounded teaspoons (8g)
Why invite a corporate spokesperson?
Dr. Satin works for the Salt Institute, which according to its web site is “dedicated to advancing the many benefits of salt….” Most folks who claim authority to deem foods good or bad have ties to somebody with a financial stake, but this is unusually blatant.
I think some of you missed the point.
Robby: they used the spokes person quote as a reference to the ongoing modern debate, then used it to seqway to a discorse on the corrilation between modern science and traditional eating habbits. I hate to troll here but you comment has me wondering if you read the article.
John: Are you seriously splitting hairs over the size of a teaspoon when the article clearly states that we have no point of refrence for an upper limit but it looks like we definatly need more salt in our diet. Your complaint sounds like someone afraid of an overdose. They give a pritty big window so making an issue over salt density and wether or not things are slightly rounded or flat is something of a moot point when looking at the information presented.
Caryn: Thank you for bringing up a valid issue. I would love to know the difference in health benefits between sodium cloride and sea/mineral salts on the human body, especialy their effects on blood bressure as I have had several clients in the past with that question and issue. Does anyone down the line have info or opinion on the subject?
What quote? It’s the entire article, the Salt Institute guy wrote, not just a quote.
Best quantity of salt to consume daily
Hi,
I paste my previous comment below and rev3eal a serious misunderstanding re the best Hygienic amount to take spilling hairs definitely not !
To cut a long story short (I paste the whole explanation under) It turns out that the stated amounts as suitable on an average basis is 1.5 teaspoons. This in fact relates to 12.5 grams, when In fact I believed it related to 4.5 gram, and therefore I was under dosing significantly and struggling with low BP and fatigue. How come such a discrepancy ! I live in UK and Asia and the same probably applies to Europe and possibly other countries, our teaspoon is 3 mls. If we use a bigger teaspoon in our calculations we say 5ml medicinal teaspoon to clarify. Furthermore the density of unrefined salt I have here and it is quite fine is 1. I turns out that the salt calculations suggested in the article was based on refined salt, and I have been informed by the author this has a density of 2 (will pop down the shops in a minute and purchase some to test this !) So 5ml x 1.5 teaspoons x 2 = 15 grams …a lot more than 4.5 g So splitting hairs not so !!
salt amount daily
written by John Claydon, Jun 02 2012
I think the advice about how much salt daily (as well as to use as much as possible unrefined sea salt, preferably Celtic salt) to use should be clarified thus:
A very slightly rounded teaspoon (it may appear as level to most people you actually have to shake some off to really get a level teaspoon) actually contains 4 grams. This is consistent with the fact that the density of salt is is higher than 1. Fairly fine grain Celtic salt comes in at a density of 1.1 , but finer salts would be more dense.
It should also be stated that the teaspoon we are referring to is a common (small) domestic teaspoon that can hold 3 ml of water whereas the larger medicinal teaspoon can hold 5 mls water.
In summary then I suggest the daily amount recommended, if we are talking about teaspoons should state: Suggested use from a slightly rounded (common 3 ml) teaspoon (approx 4 g) to 2 slightly rounded teaspoons (8g) ….
So what I wrote here on June 02 2012 was evidence of a understandable misunderstanding…… the amount is even higher as we have now been told it relates to refined salt with an estimated density of 2 (I want to check this out as it may have just been taken from theoretical perfectly dry compressed salt-lets see what’s in the shop !
So in summary, and this especially important for people who are health conscious and not eating processed food and plenty of fruit and veg and been scared off salt years ago 10 to 14 grams a day seems an outrageous amount ! Yet I accept this seemingly mind blowing fact and am watching my health improve using about 10 to 12 grams a day of unrefined salt. In order to get this much into me each day I have to add to my teas, water and anything else that gets into my mouth ! as I don’t eat much and make all own bread etc.
D.Hom
Dear Editor of Morton Satins article,
Morton has asked me to ask the editor at Western Price to add a clarifying ‘legend table’ that converts the SI units to the more common measures used in major geographical regions around the globe. It can also refer to differences in the various types if salt used in those areas to account for sodium chloride content and density. In that way, the article can revert to the original exclusive use of SI units and the assumption of 99.99% purity NaCl found in commercial evaporated salt
Quoting from Morton Satins article
Because salt is essential to good health, the human body is hard-wired with an innate salt appetite. Around the world, population salt intakes vary somewhat, but nearly all fall within what eminent medical researcher Bjørn Folkow termed the “hygienic safety range” of sodium intake, between 2,300 mg/day (Salt=5.8g) and 4,600 mg/day ( 11.7g salt) ( or even 5,750 mg/day.= 14.6g salt )
In common English measures, that would be one to two or two and a half teaspoons of salt per day
Or at the start of the article exposing Mainstream Myths
by Morton Satin, PhD, Vice President,
Science and Reseach, The Salt Institute
A side from water, salt (sodium chloride) is the most ubiquitous food ingredient consumed by humankind. It is a nutrient that is essential to life and good health and has always been the predominant positive ion in extracellular body fluid for all multi-cellular animals.
Having originally evolved from a marine environment, the human body’s salt-to-water ratio is critical to metabolism. Human plasma contains 0.9 percent sodium chloride, most of it coming from food and a small amount from water. The fundamental indicator of salt intake sufficiency points to 1.5 teaspoons of salt per day as the basic human requirement.
This is what has led to some confusion and Morton concurs.
What Morton is referring to is 5ml teaspoons and noted that it will depend on the type i.e. the density of the salt.
I suggest that the facts be relayed simply and clearly as e.g. I have laid out below or similar for lay persons including old grannies across the world !
I found that freshly opened refined salt has a density of 1.4
I found that fine grain Celtic salt has a density of around 1.0
(A course grained sea alt would have a lower density)
The hygienic safety range is:
5.8 gram salt absolute minimum (some writers say it should be as high as 8g) up to 14.6 gram daily
For Fine grain unrefined salt: (with a density of 1.4 )
Using a 5 ml spoon as a measure
1 x 5ml spoon =5 grams
2 x 5ml spoon = 10 grams
3x 5ml spoon = 15 grams
Average suggested use refined salt 2 x 5 ml spoons a day in all food and drink (But please revert to unrefined salt ASAP)
Using the standard domestic 3 ml spoon that is the most common teaspoon used in ASIA and UK and I think Europe (If we use a 5ml teaspoon this is referred to as a medicinal teaspoon)
For unrefined fine grain sea salt e.g Celtic Salt
2 level 3 ml teaspoons = 6 grams
5 level 3 ml teaspoons = 15 grams
Average Use suggested 3 to 4 x 3ml level teaspoons daily spread across all food and drink daily
The idea of adding inorganic sodium chloride (in any form) to food, is the corporate food industry’s dream of making billions, by getting people to believe the myth that the toxic pollutant known as table salt is a must to consume.
Organic sodium from plant based foods is essential for life, sodium chloride that exists outside of the body is non essential. This article above is corporate sponsored junk, just like the food it produces.
Hi there, I would like permission to share your article on salt on my web page. I would use some excerts and then add a link to your page. My product is fermented vegetables in Australia and as you can imagine there is a lot of convern about the salt content.. If you’ve got a condensed version I can share pls let me know..
Thanks
griz
You are welcome to link to any article on the site and take excerpts from those articles. We prefer you not copy the whole article. We don’t have a condensed version, sorry.
It is astonishing that websites, supposedly with personnel who should know better, use the terms “salt” and sodium as if they were synonymous. They aren’t interchangeable terms, which is why this article needs to be re written with a proper understanding that essential organic sodium and toxic salt (sodium chloride) do not represent the same ionic metabolic responses in the body. After all, nutritive qualities ought to be the important observations, not a corporate desire to confuse the issue, by pretending that NaCl is essential to the body, it is not and millions around the world have, and still do live without sodium chloride.
SALT IS AN ESSENTIAL NUTRIENT
How can anyone consider this a proper study when the writers contradict themselves with glaringly obvious inconsistency. Two paragraphs from this study offer totally differing amounts in grams for a teaspoon of salt.
“In clinical studies, salt is calculated in millimoles (mmol) of sodium, where 100 mmol of sodium amounts to 2300 mg which is contained in one teaspoon (5 grams) of salt.”
“The case for setting the upper limit of salt consumption at the equivalent of 100 mmol (2,300 mg) sodium or one teaspoon (8 grams) of salt per day appeared even more problematic.”
Is a teaspoon five grams or eight grams? And where is your proof reader? lay people should not have to correct you.
Why use a corporate spokesperson to talk about salt, when his sole job is to promote salt for his corporate clients? Bizarre Weston-Price!!!
I don’t know about taking the advice of a spokesperson of the salt institute with the first name Morton, bur it probably carries more truth than the newly revised 2015 Dietary Guidlines for Americans. Prohibition was a success compared to the damage done to the population of the USA and world by this government effort started in 1980 after the 1977 McGovern Commison report. George McGovern at the time was on the Pritikin Diet and the guidelines were written by a vegan McGovern staffer. They buoght into the Dr. Ancel Keys lipid-cholesterol hypothesis which was never proven and was wrong.
Himalayan Crystal Salt is the most beneficial, cleanest salt available on the planet. It was formed about 230 million years ago where the energy of sun has dried up the original, primal sea. This crystal salt is absolutely pristine and natural, identical in composition to the ancient primal ocean. Himalayan salt is most commonly found as coarse grains, fine grains, or large blocks in Pink Dark pink and in white colors. Himalayan Pink Salt is used by holistic chefs, spas, health professionals, and individuals for its range of nutritional and therapeutic properties. Pink salt may be used in the same manner as table salt for culinary dishes and baking, but it is purer and higher in mineral content. Pink salt can be used to stimulate circulation, relax the body, lower blood pressure, sooth sore muscles, and remove toxins from the body. Mehran corporation exports all kind of salts
Thank you for writing and sharing your research in this article. Especially the parts about body wisdom, reasons for craving salt and traditional intake were helpful to me. Reminded me how domestic and wild animals absolutely need salt. Also I have been using reverse osmosis water for 3 years now, and probably was having way too little salt, because, as you described, when I dring any amount of water (reverse osmosis or otherwise) my body gets rid of it pretty fast, in a matter of seconds. I had always thought that means I am well hydrated, but when I read about salt avidity (craving), I remember having that all my life, and was always made fun of because I needed/wanted way more salt than anyone else. So I made a drink of two 200ml (1 quart each ) Water and and a teaspoon salt. And sure enough, it took an hour before it came back out. That was quite a revelation. Thank you so much!
I wonder if someone knowledgeable could comment on the connection between intake of salt (or sodium) and the body’s tendency to retain fluid. I suffer from congestive heart failure and am advised to follow a very low sodium diet (under 2000 mg/day) in order to mitigate the most troubling symptoms, including shortness of breath, and fluid accumulation in the abdomen as well as the lower extremities. I have observed in the relatively short time I’ve been following the diet that lower sodium does seem to mitigate the fluid retention and the shortness of breath is not as severe. Am I just imagining it, or does a diet higher in sodium really exacerbate these symptoms? I’d love to be able to find a way around this awful, unpalatable, bland diet, but not, of course, at the expense of my health or life. Thanks for any further input.
Chris. Look up Ray Peat. Salt energy metabolism http://raypeat.com/articles/articles/salt.shtml
Really interesting to read this! Always great to debunk myths!
Agree that sodium is absolutely necessary to maintain homeostasis in our bodies. But this article does not support how sodium affects those with a less than optimal heart function and how sodium intake affects that person. If my ejection fraction is only 30% then perhaps decreasing my fluid load by limiting my sodium intake to 2000 mg per day is a more healthy approach to sodium consumption. You mention there is no effect on BP with sodium reduction however you don’t mention the status of the cardiac function in the person whose BP is not affected by sodium intake. Would results be the same if the person being studied did not have normal cardiovascular system?
Any reply regarding my previously submitted comment?
This is a deleted comment of mine on the FB feed of nutritionfacts.org
Excuse me Michael Greger M.D, but I have genetically low blood pressure. In 1999 I had bad attack of Menieres that I was hospitalized for nearly a week, connected an intravenous machine because my electrolyte levels were way too low. If sodium is such poisonous stuff why would that have slowly pumped a saline solution into my bloodstream?
After another attack in 2003,my doctor noticed I have low blood pressure and suggested I eat some salty food. I consulted the book Lets Eat Right to Keep Fit by Adelle Davies and what do you know but she attributed Menieres to a low salt diet. Since I have bumped up my salt intake I have only had mild attacks of Menieres that have not lasted more than one night. All blood pressure tests since then have been normal.
Gee, thanks Salt Institute for teaching us that salt is so good for us, and that we should eat lots of it! I’m sure that you have provided completely unbiased information… except that you haven’t.
For instance, in MYTH 4 you claim that when Finland significantly cut back on salt intake it did not lead to any health benefits. That’s a bald-faced lie and you know it. Anyone can do the research for themselves and see that they experienced a 75 to 80 percent decrease in both stroke and coronary heart disease mortality during this timeframe. (source: http://www.ncbi.nlm.nih.gov/pubmed/17046432 )
In MYTH 5, figure 3 “InterSalt Life Expectancy” omits the data points from the four low-salt cultures and does not take into account well-known confounders like alcohol intake and BMI. If you factor those things in (which the Intersalt study authors did, and which you conveniently overlooked), the slope reverses direction (i.e. lower sodium intake is associated with longer lifespan). Anyone can look this up for themselves should they wish to.
For the sake of our collective health, I’ve spent over a hundred hours researching and fact-checking many other salt-related claims at https://rebelthoughts.org/fact-checking-the-salt-fix and I invite everyone to look at the evidence and decide for themselves. If you notice any errors or omissions I will gladly consider them.
Please take care of your health—it is the most precious thing each of us has.
I find this article interesting concerning the toxicity of salt? I am wondering if more testing needs to be done about the heavy metals in the salts? I hope others have the courage to find out 🙂
https://tamararubin.com/2020/10/how-much-lead-is-in-salt-which-salt-is-safest-to-use-for-cooking-is-himalayan-salt-safe/
Mark 9:50 NJKV
50 Salt is good, but if the salt loses its flavor, how will you season it? Have salt in yourselves, and have peace with one another.”
https://www.valerosos.com/AMERICANPRISONERSOFWAR.pdf
Weekly Ration of Salt: (aprox.) 140 grams or 20 grams per day
that works out to about 7.6 grams of sodium per day.
This was facinating. Thanks